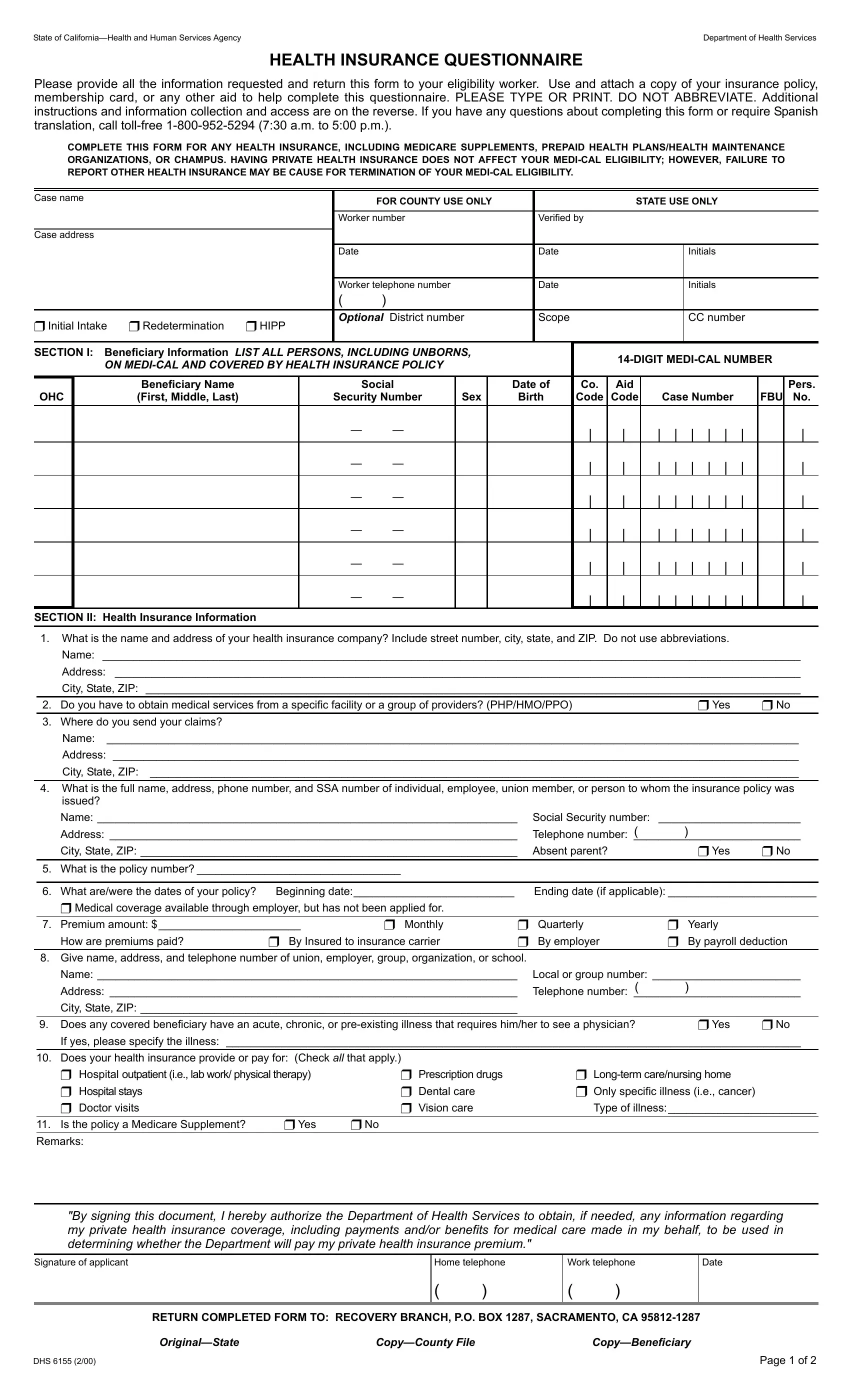
Navigating the complexities of healthcare benefits in California requires an understanding of various forms, one of which is the DHS 6155, a critical document for Medi-Cal beneficiaries. This Health Insurance Questionnaire mandates comprehensive details from applicants to ensure their eligibility for Medi-Cal benefits without being adversely affected by private health insurance plans they might also have. The form requires beneficiaries to disclose detailed personal and insurance policy information, emphasizing the necessity of reporting any other health insurance coverage as part of the eligibility evaluation process for Medi-Cal. It encompasses a range of inquiries from personal identification, such as social security numbers and Medi-Cal numbers, to health insurance specifics including policy numbers, types of coverage, and insurance providers' contact information. The document thoughtfully provides a section detailing the types of care covered by the insurance, including acute or chronic conditions, thus ensuring beneficiaries' medical needs are thoroughly assessed and addressed. Moreover, it explicitly states the requirement for Medi-Cal beneficiaries to assign rights to medical support or payments they are entitled to, from other sources, to the Medi-Cal program. This mechanism is designed to reimburse the program for expenses it covers that should have been billed to other health insurances, emblematic of Medi-Cal's role as the payer of last resort. Lastly, the form is equipped with instructions that affiliate closely with the Welfare and Institutions Code, highlighting the confidentiality of submitted information and the legal repercussions of non-disclosure, ultimately underscoring the significance of this form in the broader context of healthcare administration and patient care in California.
| Question | Answer |
|---|---|
| Form Name | Form Dhs 6155 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | state of california health questionnaire, dhs 6155 form, dhs 6155 pdf, dhs 6155 |
