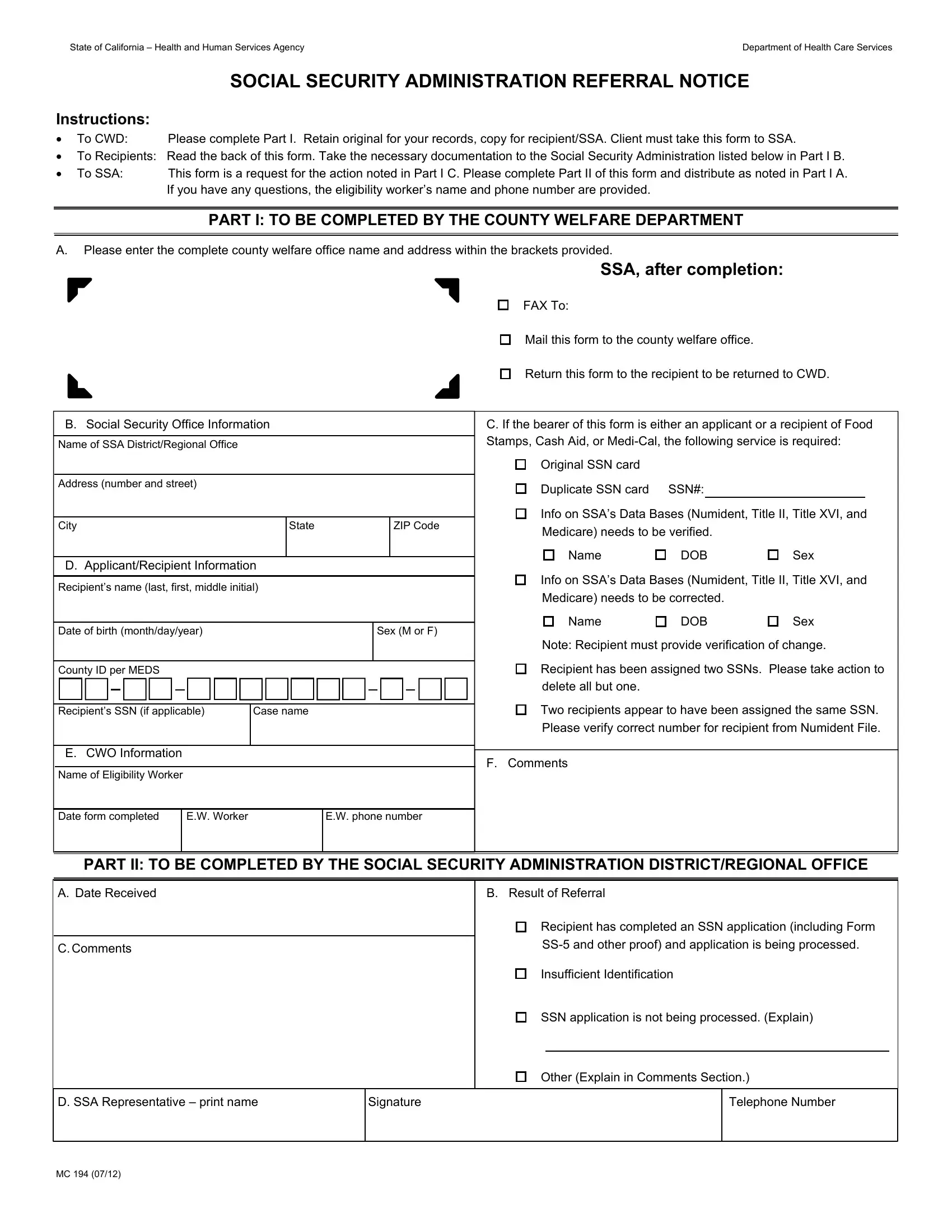
Access to Medi-Cal, CalFresh (Food Stamps), and CalWORKs in California requires a valid Social Security Number (SSN). The California MC 194 is the official referral notice used by County Welfare Departments (CWD) to communicate with the Social Security Administration (SSA). It resolves SSN discrepancies, corrections, and new SSN applications for benefit applicants and recipients. Without a valid SSN on record, individuals may face delays in receiving services they qualify for.
County Welfare Department eligibility workers (EW) complete Part I of the MC 194 referral notice. The EW enters the recipient's name, case number, and the SSN action required. Common actions include verifying an existing SSN, correcting a duplicate SSN, or requesting a new SSN. The form also provides instructions telling recipients what documents to bring to the SSA office. Required documents typically include a birth certificate, state-issued ID, or proof of immigration status. Once Part I is complete, the CWD submits the referral notice to the appropriate SSA field office for processing.
The Social Security Administration reviews the referral notice and completes Part II of the form. The SSA records the date received, the result of the referral, and any relevant comments. The outcome may confirm the SSN is verified, that a correction has been made, or that more documentation is required. Once the SSA responds, the CWD can resume processing the Medi-Cal, CalFresh, or CalWORKs application. Related Medi-Cal eligibility administration forms include California Form MC 011 and California Form MC 012, which address other aspects of health coverage eligibility.
Receiving an MC 194 notice means the county found a problem with your SSN record. You may need to visit a local SSA office with identity documents to resolve the issue. Your county caseworker or eligibility worker will explain what steps to take and how long the process will take. The MC 194 referral process upholds federal law by ensuring all state assistance applicants have verified SSN records. Individuals involved in broader Social Security processes may also need to review California Form MC 358 or complete a Social Security Application as part of their SSN establishment.
| Question | Answer |
|---|---|
| Form Name | California Form Mc 194 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | ssn, 95a, ssa, ar3a |