
canada standard dental claim form can be completed without difficulty. Simply open FormsPal PDF editor to complete the task fast. The tool is consistently maintained by our staff, acquiring powerful functions and growing to be better. If you are looking to start, here's what it will take:
Step 1: Open the PDF form inside our editor by clicking on the "Get Form Button" at the top of this page.
Step 2: With our handy PDF editor, you'll be able to accomplish more than simply fill in blank fields. Edit away and make your docs seem professional with customized text put in, or modify the original content to perfection - all that comes along with an ability to incorporate any images and sign the PDF off.
As a way to complete this form, make certain you provide the right information in every blank:
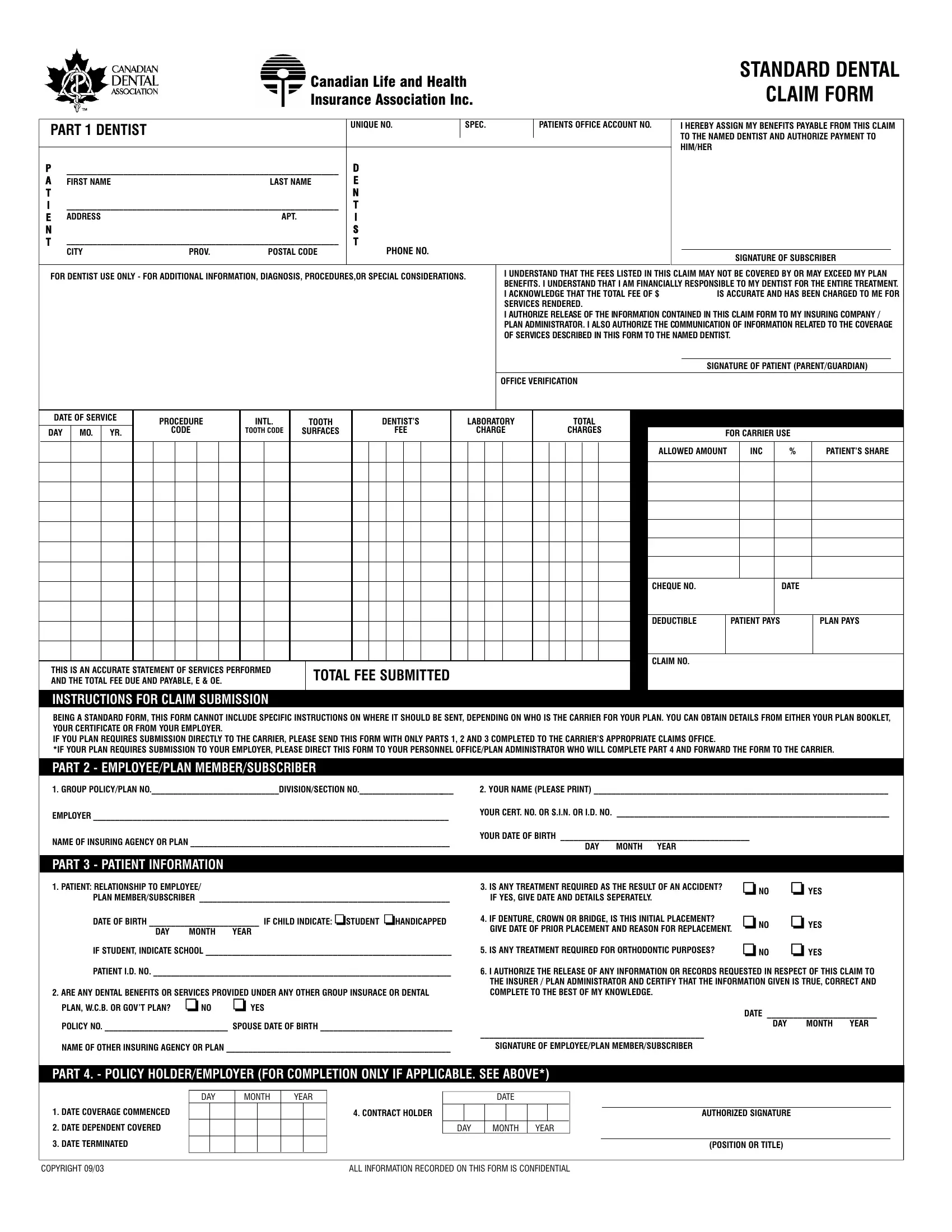
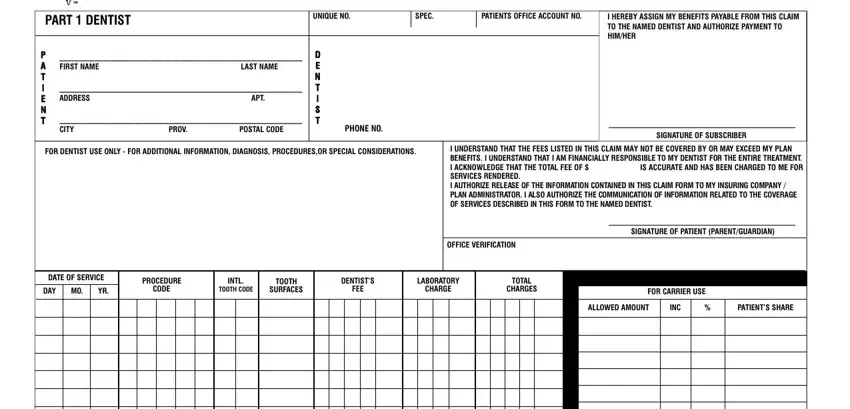
1. The canada standard dental claim form necessitates specific details to be inserted. Be sure the subsequent blank fields are completed:
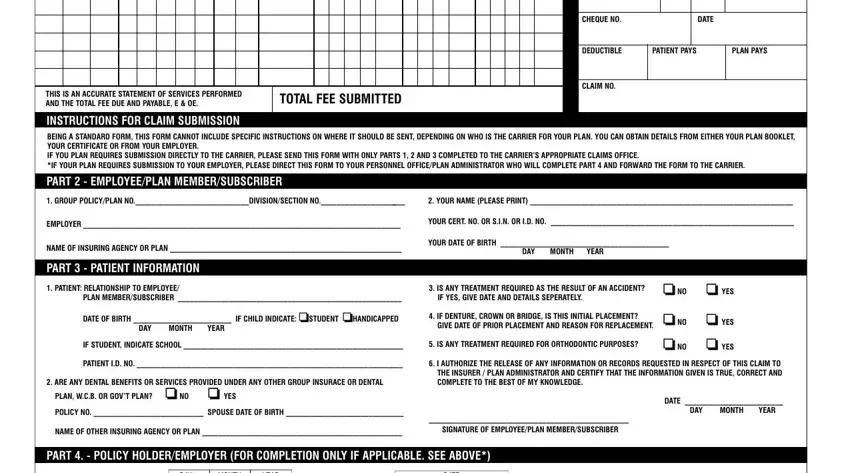
2. When the last section is completed, you have to put in the required specifics in THIS IS AN ACCURATE STATEMENT OF, TOTAL FEE SUBMITTED, CHEQUE NO, DATE, DEDUCTIBLE, PATIENT PAYS, PLAN PAYS, CLAIM NO, INSTRUCTIONS FOR CLAIM SUBMISSION, PART EMPLOYEEPLAN, GROUP POLICYPLAN, YOUR NAME PLEASE PRINT , EMPLOYER , YOUR CERT NO OR SIN OR ID NO , and NAME OF INSURING AGENCY OR PLAN allowing you to go further.
People frequently make mistakes while completing INSTRUCTIONS FOR CLAIM SUBMISSION in this area. Ensure you re-examine everything you type in right here.
3. Completing DATE COVERAGE COMMENCED, DATE DEPENDENT COVERED, DATE TERMINATED, DAY MONTH YEAR, DATE, CONTRACT HOLDER, DAY MONTH YEAR, COPYRIGHT , ALL INFORMATION RECORDED ON THIS, AUTHORIZED SIGNATURE, and POSITION OR TITLE is essential for the next step, make sure to fill them out in their entirety. Don't miss any details!

Step 3: After you have reviewed the information entered, simply click "Done" to complete your form. Acquire your canada standard dental claim form when you register online for a 7-day free trial. Easily get access to the pdf form from your FormsPal account page, along with any modifications and changes all synced! Here at FormsPal.com, we strive to guarantee that your details are kept secure.