
 No Td or Tdap
No Td or Tdap
 No
No
 No
No
 No
No
 No
No
You'll find nothing troublesome in relation to filling out the capf 31 after you open our tool. By taking these simple steps, you will get the prepared PDF in the minimum period possible.
Step 1: This page includes an orange button that says "Get Form Now". Click it.
Step 2: Right now, it is possible to alter the capf 31. This multifunctional toolbar will let you add, remove, transform, highlight, as well as perform other commands to the text and fields within the document.
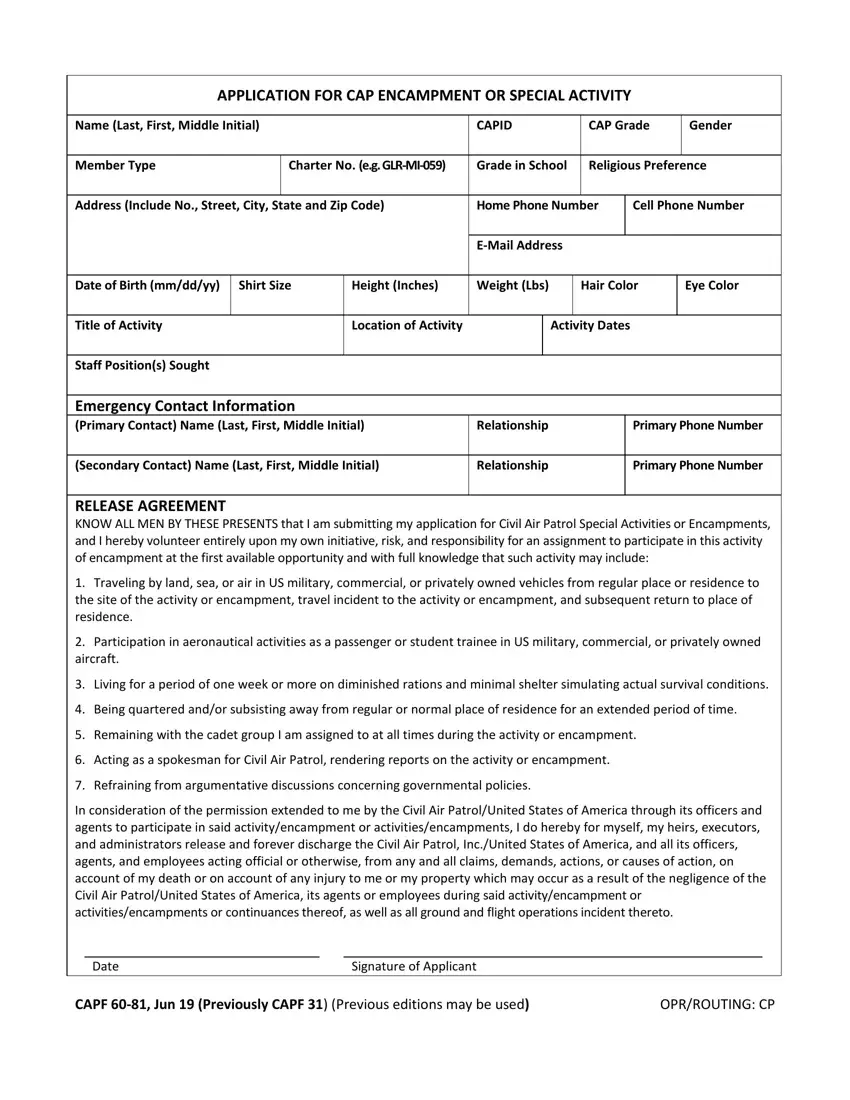
In order to fill out the file, provide the information the software will require you to for each of the following segments:
In the In consideration of the permission, Date, Signature of Applicant, CAPF Jun Previously CAPF, and OPRROUTING CP field, put in writing your details.
Within the section referring to Name Last First Middle Initial, Title of Activity, RELEASE BY PARENTS OR GUARDIAN, Is my minor child or ward, Has no history or injury or, Will follow all rules regulations, However in case of injury disease, Date, Witness for Fathers Signature, and Father or Legal Guardian, you should put down some expected information.
The Squadron Certification Squadron, Date Group Certification Group, Squadron Commander, Date Wing Certification Wing, Group Commander or designee, Date CAPF Reverse, Wing Commander or designee, and OPRROUTING CP section is the place to place the rights and obligations of each party.
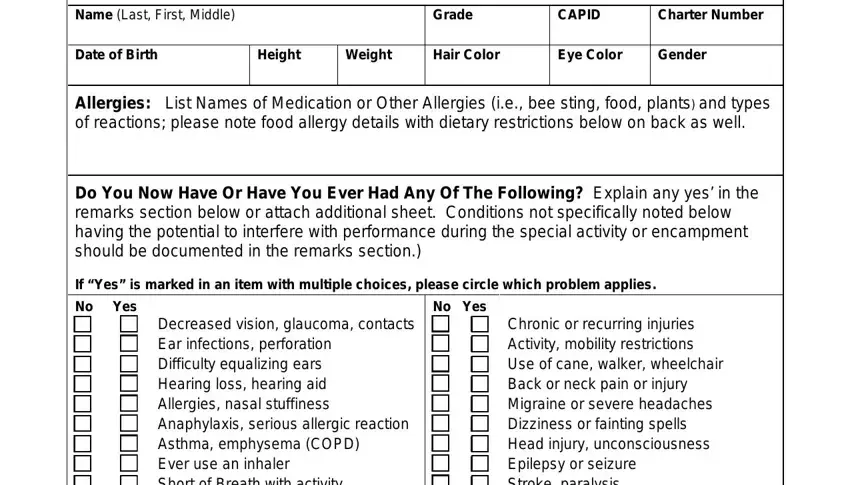
Finalize by analyzing the next areas and completing them accordingly: This information is CONFIDENTIAL, Name Last First Middle, Grade, CAPID, Charter Number, Date of Birth, Height, Weight, Hair Color, Eye Color, Gender, Allergies List Names of Medication, Do You Now Have Or Have You Ever, If Yes is marked in an item with, and No Yes.
Step 3: Once you have clicked the Done button, your document is going to be readily available upload to any electronic device or email address you identify.
Step 4: Make as much as two or three copies of the file to stay clear of any sort of possible issues.
