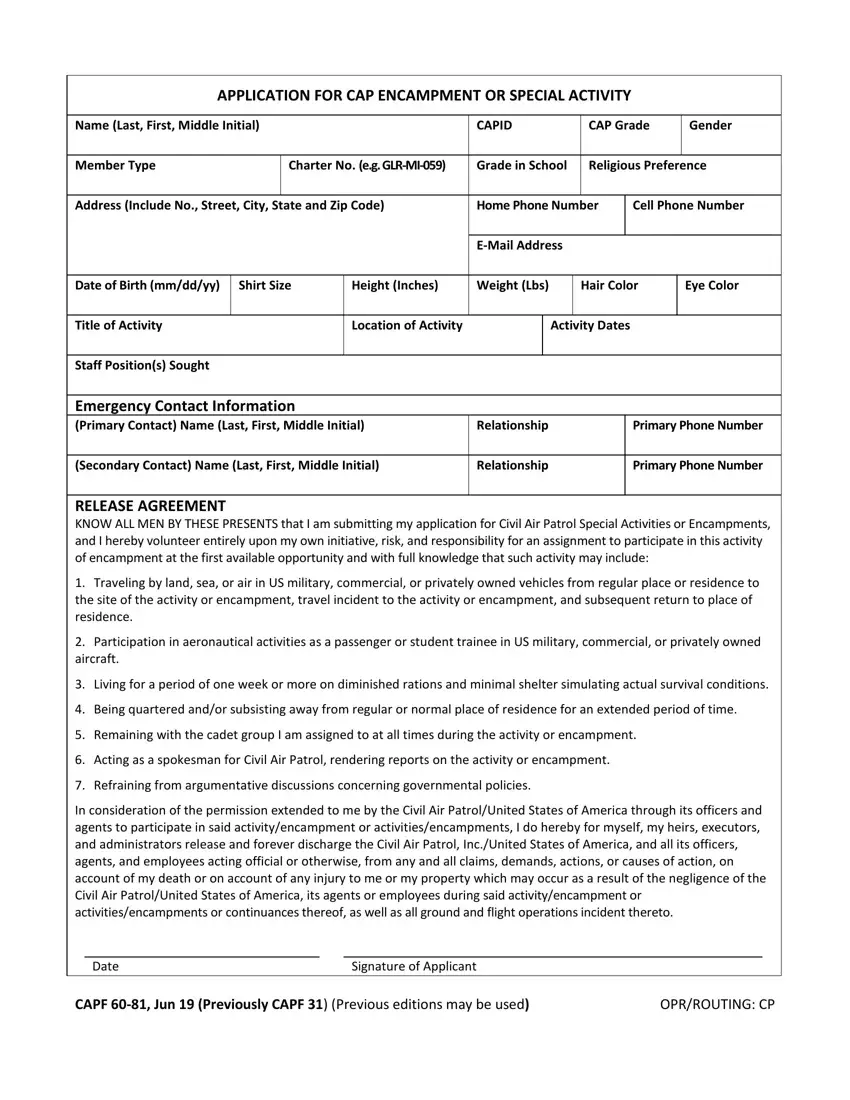
The CAP Form 31, officially titled APPLICATION FOR CAP ENCAMPMENT OR SPECIAL ACTIVITY, is the standard Civil Air Patrol application form for members joining encampments and special activities.
The form collects essential personal data: your full name, CAPID, contact details, shirt size, height, and weight. Organizers use this information to prepare appropriate resources for each participant.
A dedicated section covers medical history and emergency contact information. CAP staff review this data to handle health concerns and reach family members during the activity.
The form includes a RELEASE AGREEMENT and a RELEASE BY PARENTS OR GUARDIAN section. Both sections document the voluntary nature of participation and acknowledge the physical risks involved. Completing and signing these sections is required before a cap form 31 application is approved.
Squadron commanders and group certification officers countersign each completed form, confirming the member meets eligibility requirements for the selected encampment or special activity.
| Question | Answer |
|---|---|
| Form Name | Cap Form 31 |
| Form Length | 6 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 1 min 30 sec |
| Other names | cap form application special, civil air patrol form 31, form cap 31, application encampment |
