
There's nothing complicated about filling in the capital blue cross appeals department after you open our PDF editor. By following these simple steps, you will get the ready file in the minimum time period possible.
Step 1: Choose the button "Get Form Here".
Step 2: At the moment, you can start modifying your capital blue cross appeals department. The multifunctional toolbar is available to you - insert, delete, adjust, highlight, and undertake other sorts of commands with the text in the file.
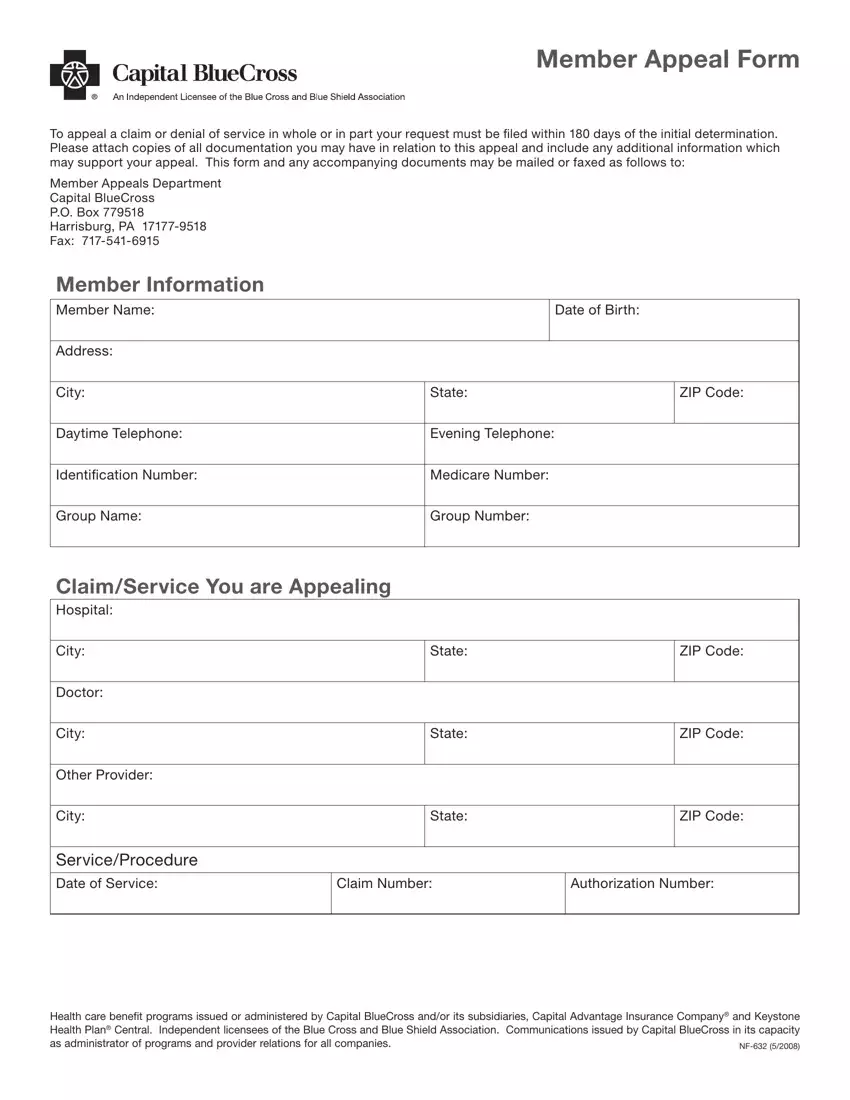
Fill out the capital blue cross appeals department PDF by entering the data meant for each individual part.
Remember to fill up the City, Other Provider, City, ServiceProcedure Date of Service, State, State, ZIP Code, ZIP Code, Claim Number, Authorization Number, and Health care benefit programs space with the necessary information.
You can be requested for certain significant data if you need to fill up the Reason for the Appeal area.
The field Member Signature, Date, If appointing someone to i le the, Authorization of Designated, Subscriber, Subscriber ID Number, Todays Date, Group Number, Section IAuthorization of, and to act as my representative in should be where you add all sides' rights and responsibilities.
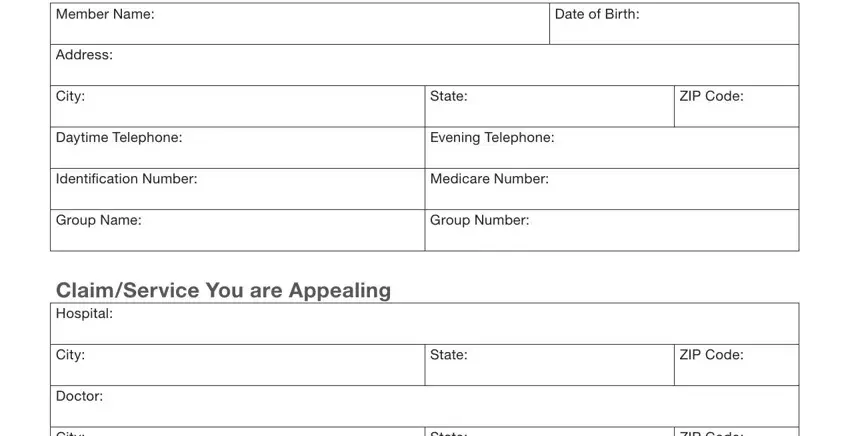
Review the sections Member Name, Address, City, Date of Birth, State, ZIP Code, Daytime Telephone, Evening Telephone, Signature of Member, Date, Section Acceptance of, hereby accept the above referenced, appointment I am aan, STATUS OR RELATIONSHIP TO THE, and of the Member and will and then fill them out.
Step 3: Click the button "Done". Your PDF form may be exported. You may download it to your device or send it by email.
Step 4: It's possible to make duplicates of the form tostay clear of any kind of future problems. Don't get worried, we cannot publish or track your information.
