There is nothing complicated about completing this Capital Blue Cross appeal document with FormsPal's PDF editor. Follow these steps to get your appeal ready to submit.
Step 1: Get Started
Choose the button "Get Form Here" to open the PDF editor in your browser.
Step 2: Fill In Your Information
You can start modifying the appeal document right away. The multifunctional toolbar is available to you - insert, delete, adjust, highlight, and undertake other commands with the text in the file.
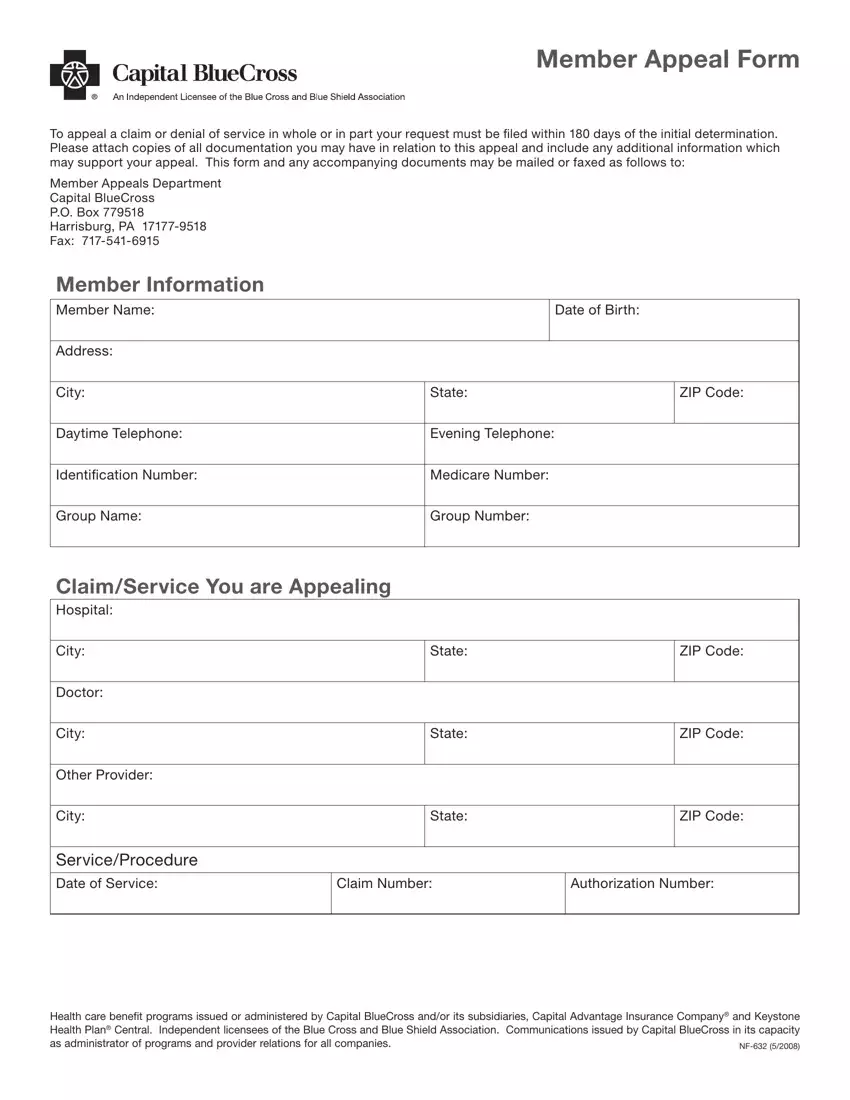
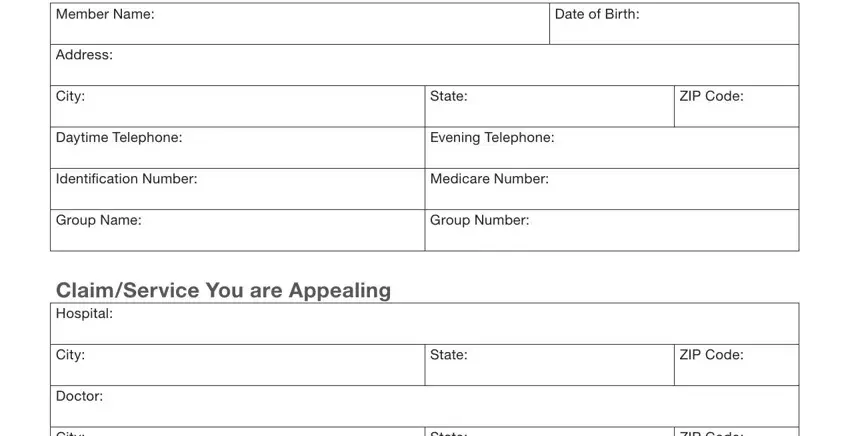
Complete each field in the appeal document by entering the data meant for each individual part.
Remember to fill in the following fields with the required information:
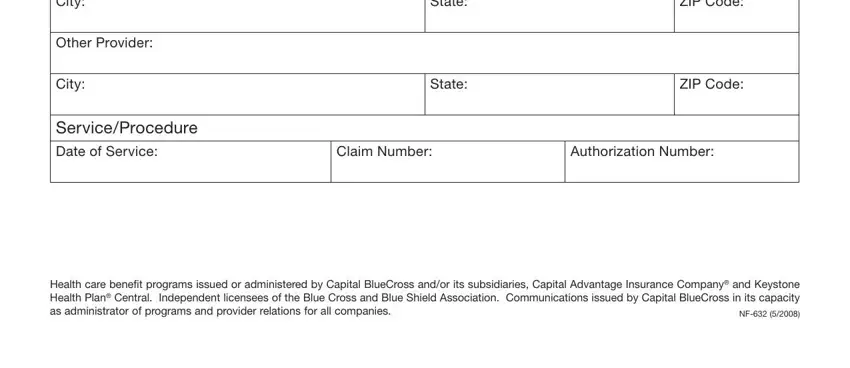
- City and State
- Other Provider
- Service or Procedure Date of Service
- ZIP Code
- Claim Number and Authorization Number
- Health care benefit programs
You may be asked for additional details when completing the Reason for the Appeal section.
The fields for Member Signature, Date, Authorization of Designated Representative, Subscriber ID Number, Today's Date, and Group Number are where you provide all parties' rights and responsibilities.
Review and complete the following acceptance fields:
- Member Name, Address, City, Date of Birth
- State, ZIP Code, Daytime and Evening Telephone
- Signature of Member and Date
- Status or Relationship to the Member
Step 3: Save and Export
Click the button "Done". Your PDF file may be exported, downloaded to your device, or sent by email.
Step 4: Keep a Copy
Make copies of this document to avoid any future issues. We do not publish or track your personal information.
Related insurance documents: Anthem Blue Cross application form, general appeal form, or health insurance appeal request.
