This PDF editor was built to be so simple as possible. If you keep to the next steps, the process of managing the proview caqh form is going to be straightforward.
Step 1: The first step requires you to hit the orange "Get Form Now" button.
Step 2: Now you're on the file editing page. You may enhance and add information to the file, highlight words and phrases, cross or check certain words, insert images, put a signature on it, delete needless fields, or remove them entirely.
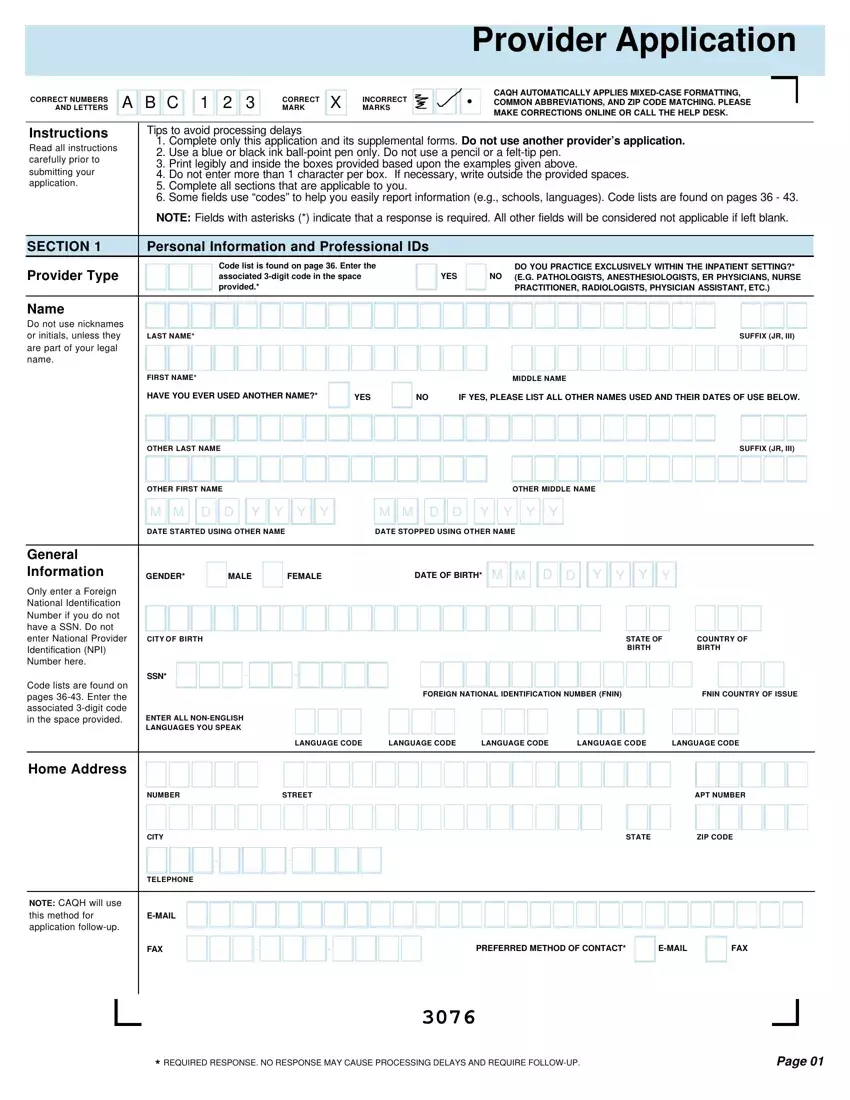
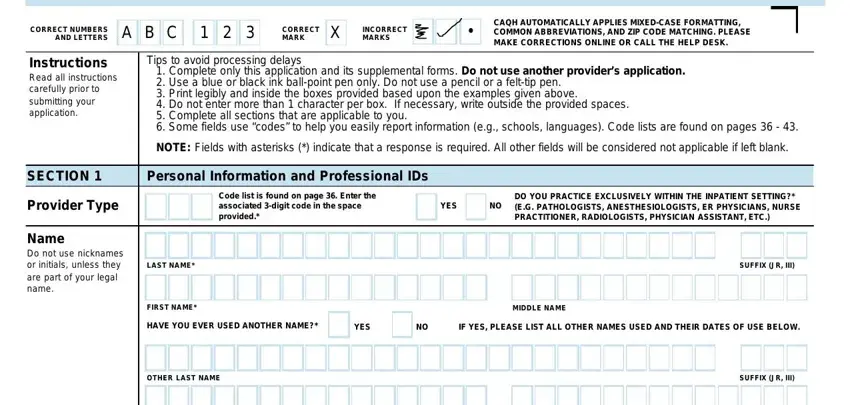
If you want to prepare the proview caqh PDF, enter the information for each of the sections:
Complete the M M D D Y Y Y Y, M M D D Y Y Y Y, DATE STARTED USING OTHER NAME, DATE STOPPED USING OTHER NAME, GENDER MALE FEMALE, DATE OF BIRTH, M M D D Y Y Y Y, CITY OF BIRTH, SSN, ENTER ALL NONENGLISH LANGUAGES YOU, STATE OF BIRTH, COUNTRY OF BIRTH, FOREIGN NATIONAL IDENTIFICATION, FNIN COUNTRY OF ISSUE, and LANGUAGE CODE area with the data demanded by the application.
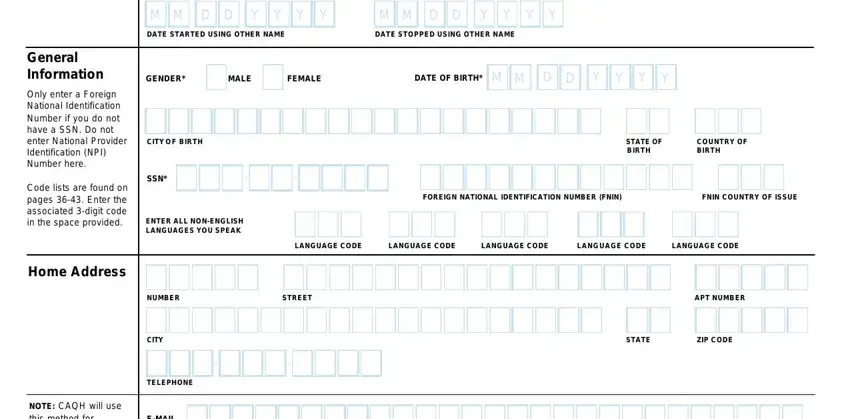
The system will demand you to give some vital info to automatically submit the segment EMAIL, FAX, NOTE CAQH will use this method for, PREFERRED METHOD OF CONTACT, EMAIL, FAX, REQUIRED RESPONSE NO RESPONSE MAY, and Page.
Spell out the rights and obligations of the parties in the section Section, Personal Information and, Professional IDs, Include all state licenses DEA, Provide all current and previous, Nonlicensed professionals should, If you have additional, FEDERAL DEA NUMBER, M M D D Y Y Y Y, DEA ISSUE DATE, M M D D Y Y Y Y, DEA STATE OF REGISTRATION, DEA EXPIRATION DATE, CDS CERTIFICATE NUMBER, and CDS ISSUE DATE.
End by taking a look at the following areas and filling them out accordingly: LICENSE EXPIRATION DATE, Code list is found on page use, Code list is found on page use, LICENSE STATUS CODE, LICENSE TYPE, ARE YOU A PART ICIPATING MEDICARE, ARE YOU A PART ICIPATING MEDICAID, YES NO, YES NO, Other ID Numbers, If you have additional, MEDICARE NUMBER, UPIN, MEDICAID NUMBER, and MEDICAID STATE.
Step 3: Choose the Done button to save the form. At this point it is accessible for export to your device.
Step 4: It will be more convenient to create copies of your file. You can rest easy that we won't publish or read your details.
