The PDF editor that you will begin using was developed by our number one software engineers. You can easily create the plan treatment authorization template file promptly and without problems with our app. Just keep up with the following guideline to get going.
Step 1: You can choose the orange "Get Form Now" button at the top of this page.
Step 2: After you have accessed the editing page plan treatment authorization template, you should be able to notice every one of the functions available for the file in the upper menu.
For you to fill in the form, enter the details the application will ask you to for each of the next parts:
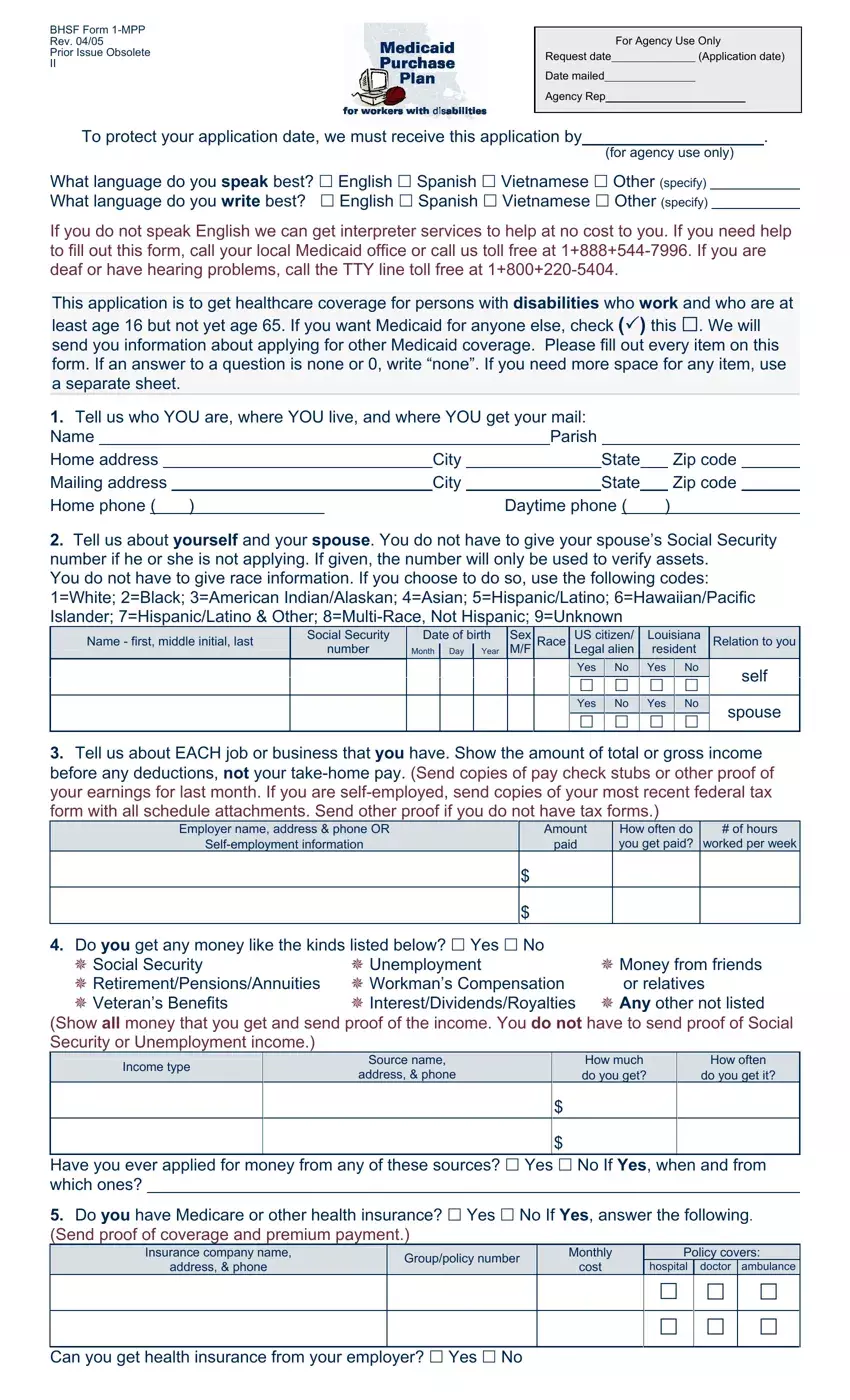
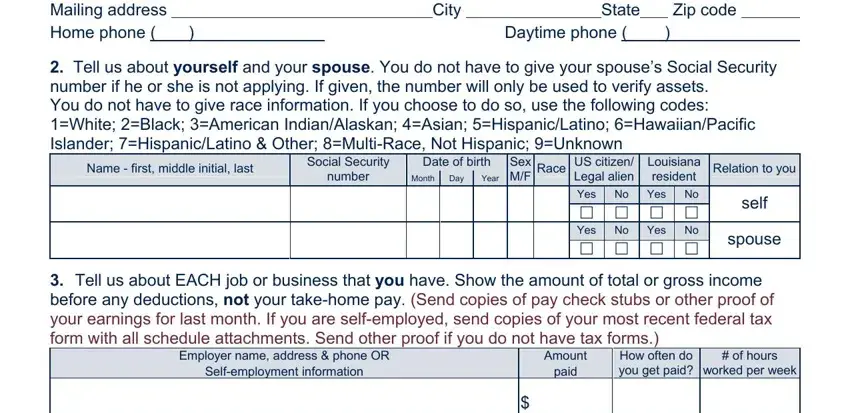
Inside the box Tell us who YOU are where YOU, Daytime phone, Tell us about yourself and your, Name first middle initial last, Social Security number, Date of birth Day, Year, Month, Sex MF, Race, US citizen Legal alien, Louisiana resident, Relation to you, Yes No Yes No cid cid cid cid Yes, and self enter the information that the platform requires you to do.
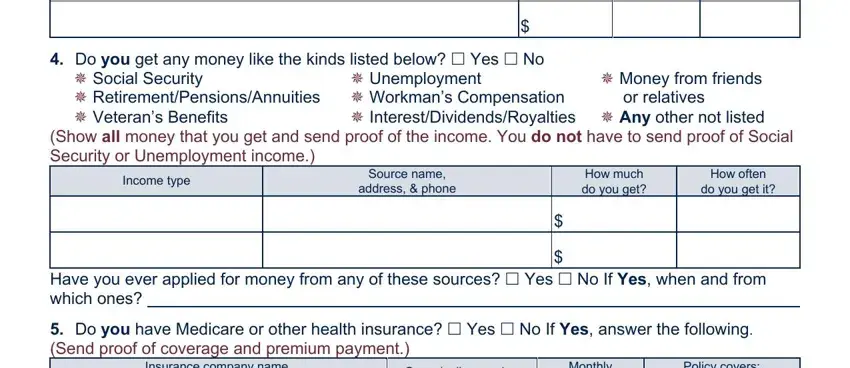
Describe the significant information in the Do you get any money like the, cid InterestDividendsRoyalties cid, cid Money from friends or relatives, cid Unemployment, Income type, Source name address phone, How much do you get, How often do you get it, Have you ever applied for money, Do you have Medicare or other, Insurance company name address, Grouppolicy number, Monthly cost, and Policy covers segment.
Inside of field Insurance company name address, Grouppolicy number, Monthly cost, Policy covers, hospital, doctor ambulance, cid cid cid, cid cid cid, and Can you get health insurance from, state the rights and responsibilities.

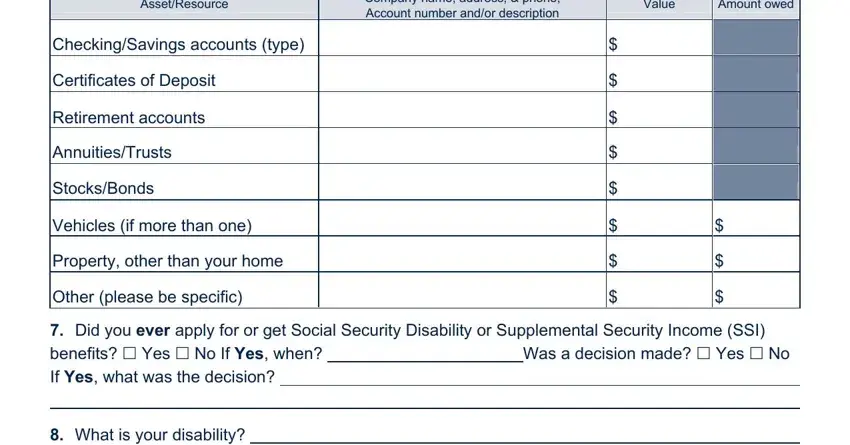
Finalize by taking a look at the following areas and completing them accordingly: AssetResource, Company name address phone, Value, Amount owed, CheckingSavings accounts type, Certificates of Deposit, Retirement accounts, AnnuitiesTrusts, StocksBonds, Vehicles if more than one, Property other than your home, Other please be specific, Did you ever apply for or get, and What is your disability.
Step 3: After you hit the Done button, your ready document can be easily exported to any kind of your devices or to email indicated by you.
Step 4: Produce copies of the document. This can protect you from possible future misunderstandings. We don't see or publish your data, for that reason be assured it will be secure.
