
What Information Does the CDL Data Form Require?
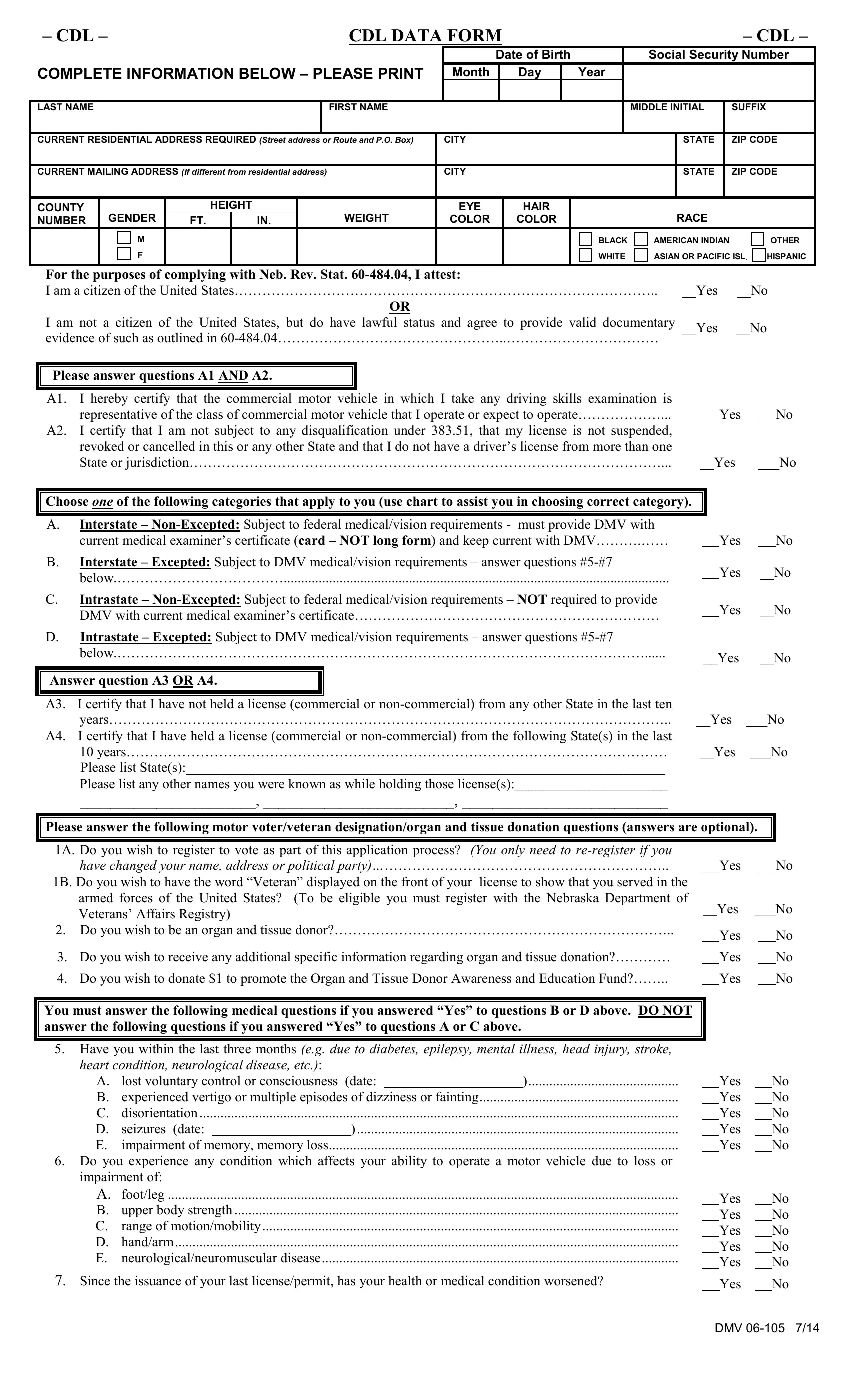
The Nebraska CDL Data Form collects several categories of personal data. You will need to provide your full legal name, date of birth, social security number, current home address, height, weight, eye color, hair color, and race. The form also requests your current driver's license number and the state that issued it. All information must match your official identification documents.
Medical Certification Categories
The CDL application includes a medical certification section divided into four categories based on the nature of your commercial driving activity.
- Category A: Non-excepted interstate. Applies to drivers operating commercial vehicles across state lines.
- Category B: Excepted interstate. For drivers who operate in interstate commerce but only transport commodities listed as excepted under federal regulations.
- Category C: Non-excepted intrastate. For Nebraska drivers who only operate within the state and do not meet federal exemptions.
- Category D: Excepted intrastate. For intrastate drivers who qualify for an exemption from federal medical standards.
Your chosen category determines which medical certification documents you must submit. If you are unsure which category applies, contact your local Nebraska DMV office before completing the form.
How to Fill Out the CDL Data Form Step by Step
- Download or open the CDL Data Form using the button above.
- Enter your full legal name as it appears on your current driver's license.
- Complete all personal information fields: date of birth, social security number, address, height, weight, and physical descriptors.
- Select your citizenship status and confirm you meet federal CDL driving qualification requirements.
- Choose the correct medical certification category based on your driving type (A, B, C, or D).
- Complete the optional fields for voter registration, veteran designation, and organ donation preference.
- Review all entries, then sign and date the completed form.
- Submit the form to your Nebraska DMV office along with any required medical certification documents.
Frequently Asked Questions About the CDL Data Form
Who needs to complete the CDL Data Form?
Any driver applying for a new CDL, renewing an existing CDL, or updating license information in Nebraska must complete this form. It is required by the Nebraska DMV for all commercial license applicants.
Can I fill out the CDL Data Form online?
Yes. Use our PDF tool above to complete and download the CDL Data Form digitally. After filling it out, print the completed form and submit it to your local Nebraska DMV office with your supporting documents.
What related CDL forms might I need?
Depending on your CDL class and endorsements, you may also need the CDL Pre-Trip Inspection Form and a Medical Fitness Certificate. Drivers applying for a vehicle registration update can also use the Vehicle Registration Application.
How long does the CDL application process take?
Completing the CDL Data Form typically takes 10 to 15 minutes. Have your current driver's license, social security card, and medical certification ready before you start. Processing time at the Nebraska DMV office varies by location.