
Who Needs to Complete This Form
The CHRC 103 is completed by an authorized representative of the hiring healthcare agency, not by the job applicant. The agency’s authorized person provides their own agency name, title, address, and contact information in the upper section of the form. They then record the identifying details of the subject individual in the next section. If you are a job applicant, your prospective employer’s HR or compliance team will complete and submit this form on your behalf.
You are able to complete this form instantly using our PDFinity® online PDF editor. We regularly release new features and improvements to make the experience as smooth as possible. Follow the steps below to get started:
Step 1: Open the PDF form in our editor by clicking the “Get Form” button at the top of this page.
Step 2: The editor gives you full control to customize the document. Add new text, correct existing entries, and insert your digital signature directly in the PDF.
The form has three main sections. Here is what to enter in each:
Section 1 – Agency Information: Enter the full legal name of your agency, street address, city, state, and ZIP code. Provide the authorized person’s first and last name, job title, telephone number with area code, and email address. The email address is used by the CHRC Unit to send status notifications about the check.
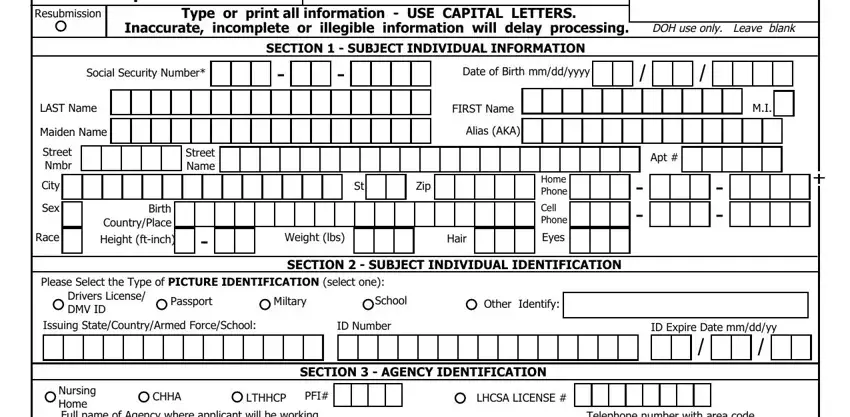
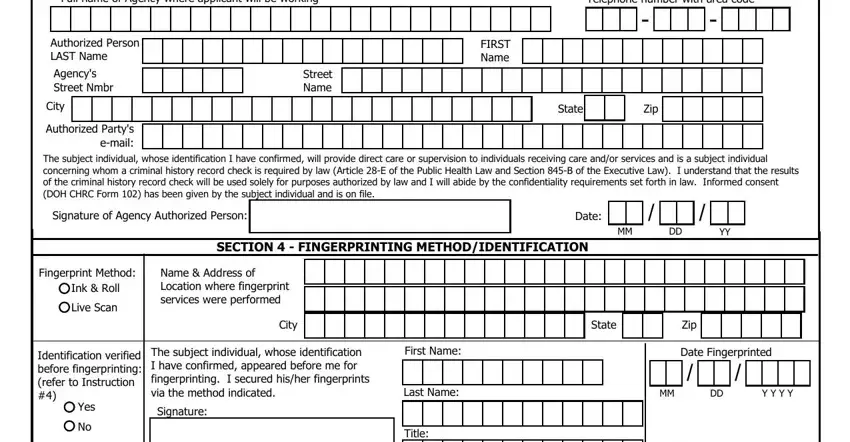
Section 2 – Subject Individual Information: This section identifies the person being checked. Enter their full name, Social Security Number, date of birth, and at least one government-issued photo ID number such as a driver’s license or passport. The authorized agency representative signs and dates this section to certify the request is for a legitimate employment purpose. The subject individual’s own signature is not required on this form.
Section 3 – Fingerprinting Information: Identify the fingerprint method used for this submission. Both ink-card and live-scan electronic fingerprinting are accepted. Enter the name and location of the fingerprint technician who collected the prints.
Pay particular attention to the Agency Full Name field and the Subject Individual’s First Name field. These are the two fields most commonly found incomplete in returned submissions. Verify them before signing and submitting.
Step 3: Once you have confirmed all fields are accurate, click “Done.” You can create a free account to download the completed form, email it directly, or access it later from your personal account page. All information entered on FormsPal.com is stored privately and securely.
After You Submit the CHRC 103
Once the completed form and fingerprint card are submitted to the NYS Department of Health’s CHRC Unit, the unit processes background checks through the New York State Division of Criminal Justice Services and the Federal Bureau of Investigation. Agencies receive an official determination stating whether the individual is cleared for employment, approved with conditions, or found ineligible for work in a regulated healthcare setting. Keep a copy of the determination letter on file as required by state regulations.
Common Questions About the CHRC 103 Form
What is the CHRC 103 form used for?
It is the official request document that authorized New York State healthcare agencies use to initiate a criminal history record check through the NYS Department of Health. The check covers both New York State criminal records and FBI federal records.
Who submits the CHRC 103?
The authorized representative of the healthcare agency fills out and submits the form. The agency must be licensed or certified under New York State Public Health Law to submit this request. Individual applicants do not submit the form directly.
What ID is needed for the subject individual?
The subject individual’s Social Security Number is required along with at least one additional government-issued ID, such as a driver’s license or passport. The agency representative records this information on the form based on documentation the applicant presents.
Is the CHRC 103 the same as the CHRC 102?
No. The CHRC 102 and CHRC 103 are related forms but serve different functions within the criminal history check process. Agencies may need both forms depending on the stage of the hiring review and the type of check being conducted.
For other forms commonly required in healthcare employment screening, see our background check consent form, fingerprint referral form, and full employment forms library.