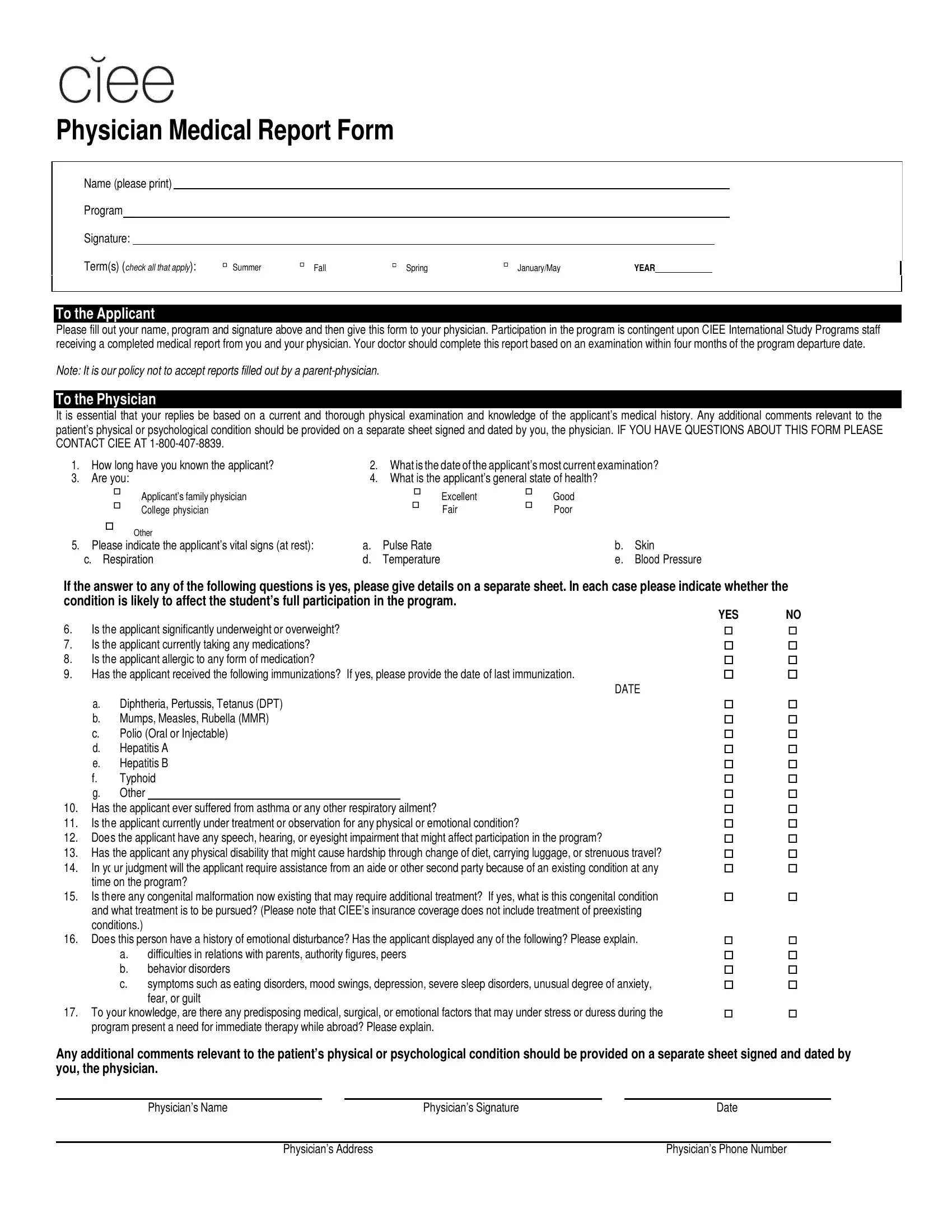
When embarking on an international study program, ensuring the health and safety of participants is paramount, and the Ciee Physician Medical Report form plays a crucial role in this process. Designed for individuals preparing to join CIEE International Study Programs, this comprehensive form serves as a bridge between the applicant's health history and the program's readiness to accommodate their medical needs. It is imperative that the applicant fills out their portion of the form, which includes basic personal information and program details, before handing it over to their physician. The physician's part delves into an in-depth medical evaluation based on a recent examination—ideally within four months of the program's start date—and a thorough review of the applicant’s medical history. Questions range from the applicant's general state of health, vital signs, and any current medications to their immunization records, any physical or emotional conditions being treated, and potential health concerns that might affect their program participation. A distinct policy against accepting reports filled out by a parent who is a physician emphasizes the importance of an objective medical assessment. Additional comments regarding the applicant's physical or psychological conditions are encouraged on a separate sheet, ensuring a holistic view of the applicant’s health. Through this meticulous process, CIEE aims to foster a safe and inclusive environment for all participants, addressing any medical needs proactively.
| Question | Answer |
|---|---|
| Form Name | CIEE Physician Medical Report Form |
| Form Length | 1 pages |
| Fillable? | Yes |
| Fillable fields | 62 |
| Avg. time to fill out | 12 min 43 sec |
| Other names | physician's report form, labacorp physician order pdf, medical forms price decrease, ciee medical report |
Physician Medical Report Form
Name (please print)
Program
Signature:
Term(s) (check all that apply): |
Summer |
Fall |
Spring |
January/May |
YEAR |
To the Applicant
Please fill out your name, program and signature above and then give this form to your physician. Participation in the program is contingent upon CIEE International Study Programs staff receiving a completed medical report from you and your physician. Your doctor should complete this report based on an examination within four months of the program departure date.
Note: It is our policy not to accept reports filled out by a
To the Physician
It is essential that your replies be based on a current and thorough physical examination and knowledge of the applicant’s medical history. Any additional comments relevant to the patient’s physical or psychological condition should be provided on a separate sheet signed and dated by you, the physician. IF YOU HAVE QUESTIONS ABOUT THIS FORM PLEASE CONTACT CIEE AT
1. |
How long have you known the applicant? |
2. |
What is the date of the applicant’s most current examination? |
||||
3. |
Are you: |
|
4. |
What is the applicant’s general state of health? |
|||
|
|
Applicant’s family physician |
|
|
Excellent |
|
Good |
|
|
|
|
|
|||
|
College physician |
|
Fair |
Poor |
|||
|
|
|
|
|
|||
|
Other |
|
|
|
|
5. Please indicate the applicant’s vital signs (at rest): |
a. |
Pulse Rate |
b. |
Skin |
|
c. Respiration |
d. |
Temperature |
e. |
Blood Pressure |
|
If the answer to any of the following questions is yes, please give details on a separate sheet. In each case please indicate whether the condition is likely to affect the student’s full participation in the program.
|
|
YES |
NO |
6. |
Is the applicant significantly underweight or overweight? |
|
|
7. |
Is the applicant currently taking any medications? |
|
|
8. |
Is the applicant allergic to any form of medication? |
|
|
9. |
Has the applicant received the following immunizations? If yes, please provide the date of last immunization. |
|
|
|
|
DATE |
|
a.Diphtheria, Pertussis, Tetanus (DPT)
b.Mumps, Measles, Rubella (MMR)
c.Polio (Oral or Injectable)
d.Hepatitis A
e.Hepatitis B
f.Typhoid
g.Other
10.Has the applicant ever suffered from asthma or any other respiratory ailment?
11.Is the applicant currently under treatment or observation for any physical or emotional condition?
12.Does the applicant have any speech, hearing, or eyesight impairment that might affect participation in the program?
13.Has the applicant any physical disability that might cause hardship through change of diet, carrying luggage, or strenuous travel?
14.In yo ur judgment will the applicant require assistance from an aide or other second party because of an existing condition at any time on the program?
15.Is there any congenital malformation now existing that may require additional treatment? If yes, what is this congenital condition and what treatment is to be pursued? (Please note that CIEE’s insurance coverage does not include treatment of preexisting conditions.)
16.Does this person have a history of emotional disturbance? Has the applicant displayed any of the following? Please explain.
a.difficulties in relations with parents, authority figures, peers
b.behavior disorders
c.symptoms such as eating disorders, mood swings, depression, severe sleep disorders, unusual degree of anxiety, fear, or guilt
17.To your knowledge, are there any predisposing medical, surgical, or emotional factors that may under stress or duress during the program present a need for immediate therapy while abroad? Please explain.
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Any additional comments relevant to the patient’s physical or psychological condition should be provided on a separate sheet signed and dated by you, the physician.
Physician’s Name |
Physician’s Signature |
Date |
|
|
|
|
Physician’s Address |
Physician’s Phone Number |