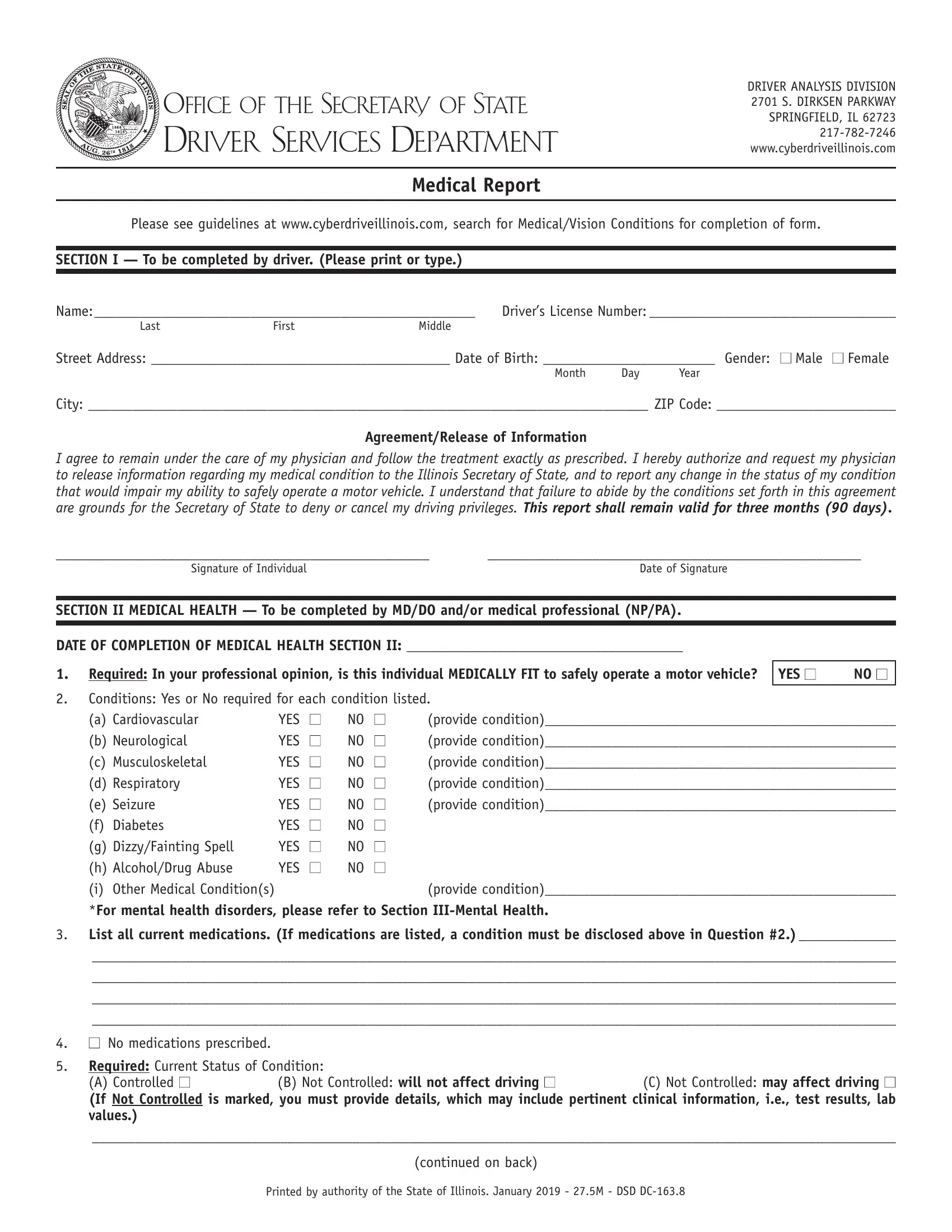
Ensuring the safety of all drivers on the road involves a complex interplay of regulations, one of which includes the Medical Report form, a document as critical as it is comprehensive, issued by the Illinois Secretary of State's Driver Services Department. This form serves a fundamental purpose: to ascertain an individual's medical fitness to operate a vehicle safely. It meticulously gathers information, starting with personal details supplied by the driver, encompassing a wide range of medical conditions from cardiovascular to neurological issues, and extending to include essential data on any medications prescribed. Notably, the form delves into the realms of both physical and mental health, requiring detailed assessments from medical professionals. It emphasizes the importance of ongoing medical supervision and underscores the driver’s responsibility to adhere to their treatment plans. The form stands as a testament to the state's commitment to road safety, demanding honest and thorough evaluations to protect the driver and the broader community. With such a rigorous approach, the Medical Report form plays a pivotal role in navigating the complexities of health-related driving eligibility, making it an indispensable tool for maintaining the highest standards of road safety in Illinois.
| Question | Answer |
|---|---|
| Form Name | Medical Report Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | illinois driver's license re examination form, elodie cheyssac, illinois medical report, medical report pdf |