Completing the CMS 116 form is easy with our PDF editor. Follow these steps to prepare the document right away.
Step 1: On this web page, select the orange "Get form now" button.
Step 2: Now you can edit the form. You have a wide range of options thanks to our toolbar. You can add, erase, or customize the content, highlight sections, and perform other editing tasks.
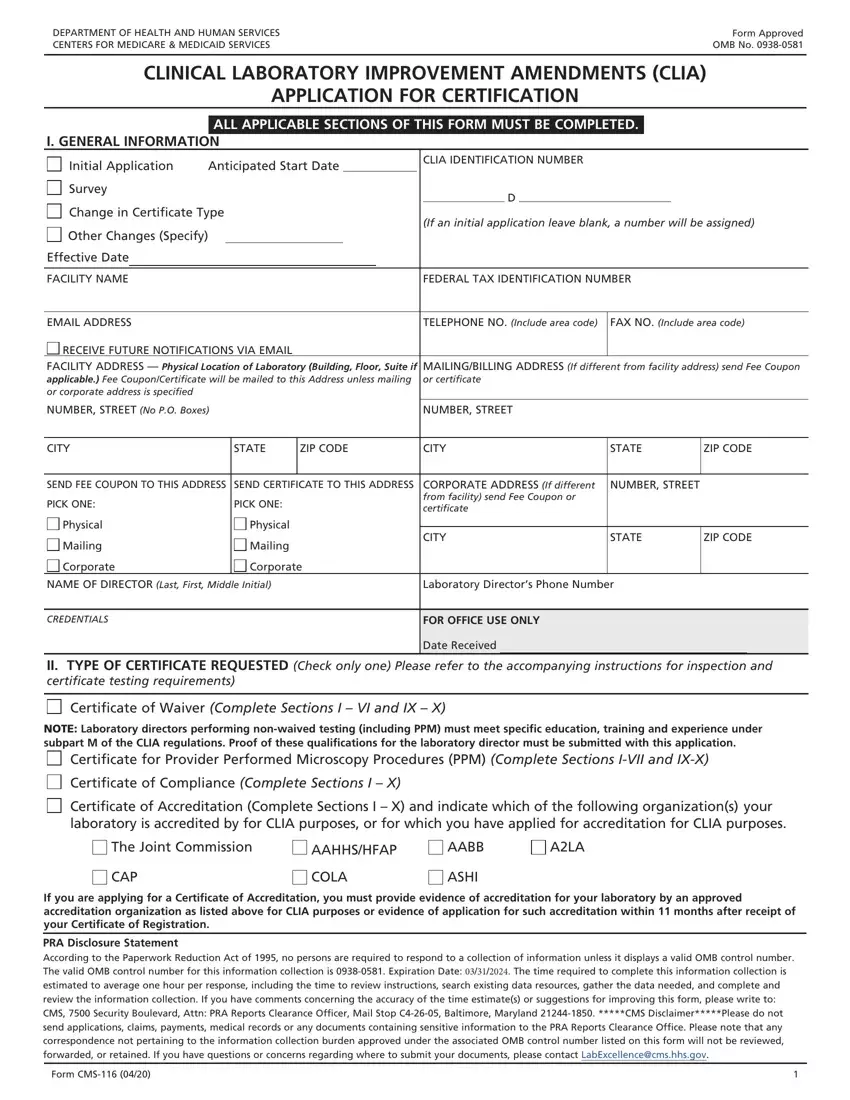
To fill in the form, enter the information for each of the following sections:
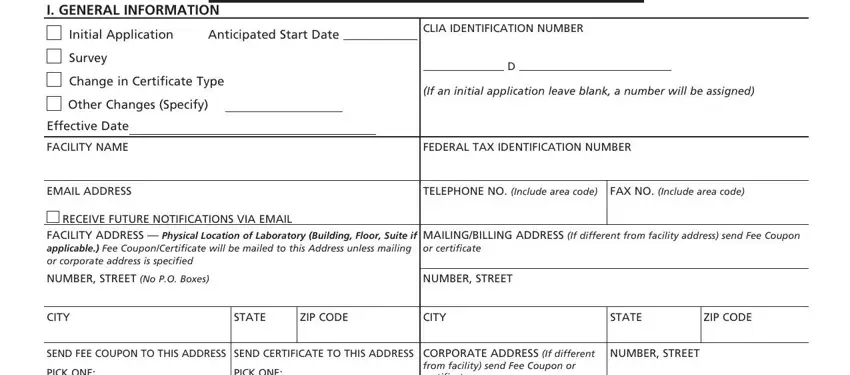
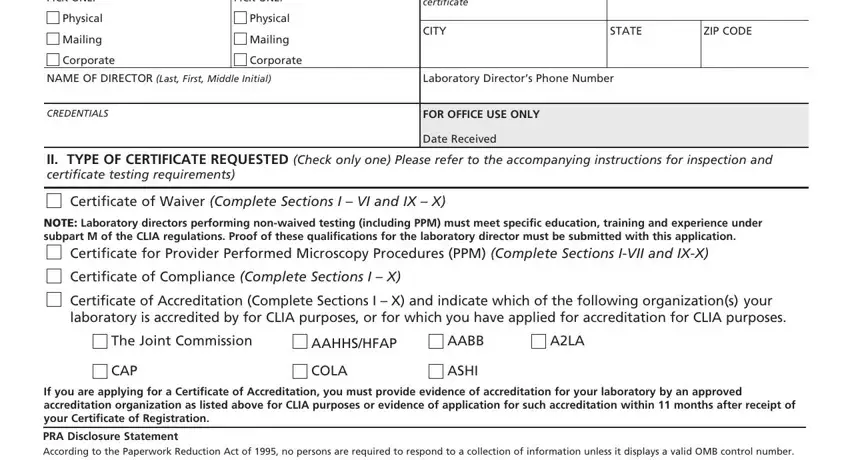
In the PICK ONE, CORPORATE ADDRESS, Physical, Mailing, Corporate, CITY, STATE, ZIP CODE, NAME OF DIRECTOR Last First Middle, Laboratory Directors Phone Number, and CREDENTIALS fields, enter the details the application requires.
Provide information in Box III TYPE OF LABORATORY, including options such as Ambulance, Ambulatory Surgery, Dialysis Facility, Home Health Organization, Independent, Industrial, Insurance, Practitioner, Prison, Public Health, Nursing Facility, and Tissue Bank. Also complete Section IV HOURS OF LABORATORY TESTING for each day of the week.
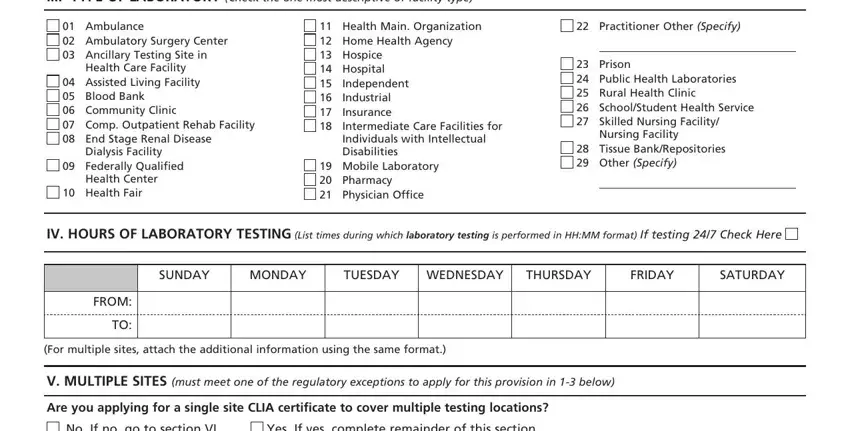
The mobile unit, non-profit status, multi-site information, and hospital department sections let applicants describe their operational details. Fill in NAME AND ADDRESS/LOCATION and TESTS information as required.
Complete the ADDRESS/LOCATION Number Street, CITY STATE ZIP CODE, TELEPHONE NO (include area code), and Form CMS fields in the final sections.

Step 3: Click the "Done" button. You can download the completed PDF to your device or send it by email.
Step 4: Save at least two copies of the form for your records.
Related CMS Laboratory Forms
If you are working on CLIA certification, you may also need these related forms:
- CMS-209 Laboratory Personnel Form - used to document laboratory director and testing personnel qualifications
- CMS-2567 Statement of Deficiencies - the form State Agencies use when noting deficiencies during a CLIA survey
Frequently Asked Questions About Form CMS-116
Who must submit Form CMS-116?
Any facility that performs laboratory testing on specimens from the human body for health assessment, diagnosis, or treatment must obtain CLIA certification. This includes hospital labs, physician offices, independent labs, nursing facilities, and clinics. Each separate location requires its own application.
What is the difference between a CLIA certificate of waiver and a certificate of compliance?
A Certificate of Waiver applies to laboratories performing only simple, low-risk waived tests. A Certificate of Compliance is required for labs performing moderate- or high-complexity tests and is issued after the laboratory passes an on-site survey conducted by the State Agency or a CMS-approved accreditation organization.
How long does CLIA certification take after submitting the form?
After submitting a complete application, CMS typically processes it within 45 to 60 days. Laboratories may receive a Certificate of Registration first, which allows them to begin testing while the full review is under way.
Where do I submit the completed CLIA application?
Submit the completed form to the State Agency in the state where the laboratory is located. Contact information for each State Agency is available on the CMS website. Some states also accept electronic submissions through the CMS online portal.
