 Yes
Yes  No Have you ever surrendered a license to practice any health care related profession in Florida or in any other state, jurisdiction or country while any such disciplinary charges were pending against you?
No Have you ever surrendered a license to practice any health care related profession in Florida or in any other state, jurisdiction or country while any such disciplinary charges were pending against you? Yes
Yes  No Do you have disciplinary action pending against any license?
No Do you have disciplinary action pending against any license? Yes
Yes  No Have you been convicted of, or entered a plea of guilty or nolo contendere, regardless of adjudication, to a felony under Chapter 409, F.S. (relating to social and economic assistance), Chapter 817, F.S. (relating to fraudulent practices), Chapter 893, F.S. (relating to drug abuse prevention and control) or a similar felony offense(s) in another state or jurisdiction?
No Have you been convicted of, or entered a plea of guilty or nolo contendere, regardless of adjudication, to a felony under Chapter 409, F.S. (relating to social and economic assistance), Chapter 817, F.S. (relating to fraudulent practices), Chapter 893, F.S. (relating to drug abuse prevention and control) or a similar felony offense(s) in another state or jurisdiction?




 Yes
Yes  No
No No
No Yes
Yes  No If “Yes” to 2, has it been more than 15 years before the date of application since the sentence and any subsequent period of probation for such conviction or plea ended?
No If “Yes” to 2, has it been more than 15 years before the date of application since the sentence and any subsequent period of probation for such conviction or plea ended? No Have you ever been terminated for cause from the Florida Medicaid Program pursuant to Section 409.913, Florida Statutes?
No Have you ever been terminated for cause from the Florida Medicaid Program pursuant to Section 409.913, Florida Statutes? Yes
Yes  No Have you been in good standing with a state Medicaid program for the most recent five years?
No Have you been in good standing with a state Medicaid program for the most recent five years? Yes
Yes  No Did the termination occur at least 20 years before to the date of this application?
No Did the termination occur at least 20 years before to the date of this application? Yes
Yes  No Are you currently listed on the United States Department of Health and Human Services' Office of Inspector General's List of Excluded Individuals and Entities?
No Are you currently listed on the United States Department of Health and Human Services' Office of Inspector General's List of Excluded Individuals and Entities?

 Yes
Yes  No
No Yes
Yes  No
NoFilling out documents along with our PDF editor is more straightforward compared to nearly anything. To edit cna reciprocity the form, there is little you will do - basically proceed with the actions below:
Step 1: Click the "Get Form Now" button to begin the process.
Step 2: Once you've entered your cna reciprocity edit page, you will notice all functions it is possible to undertake regarding your file in the upper menu.
Provide the appropriate content in each one section to complete the PDF cna reciprocity
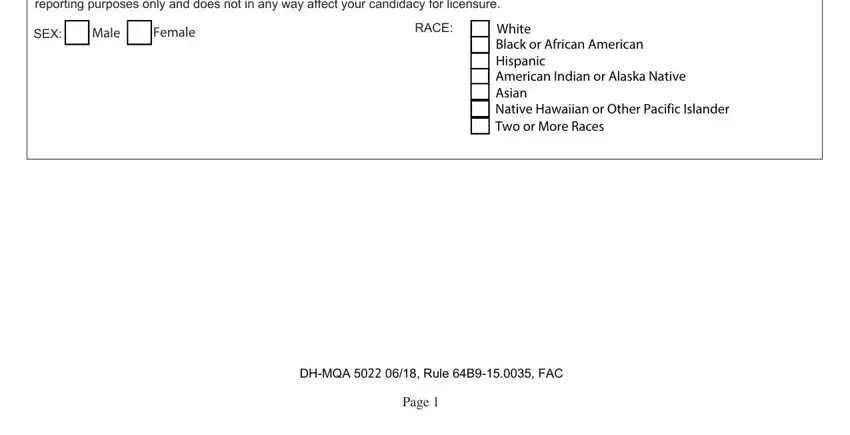
You have to fill out the EQUAL OPPORTUNITY DATA We are, SEX, Male, Female, RACE, White Black or African American, DHMQA Rule B FAC, and Page box with the required particulars.
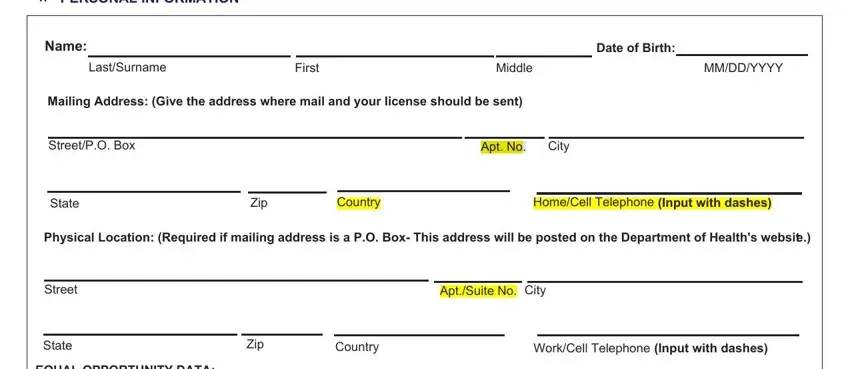
Determine the crucial details in the NAME, If you want to be notified of the, mqacnaflhealthgov, I want to be notified by email, Yes, Email Address, Under Florida law email addresses, APPLICANT BACKGROUND, Attach additional sheets if, A List any other names by which, B What names did you use when you, C What name did you use when you, Have you ever applied for, and Date part.
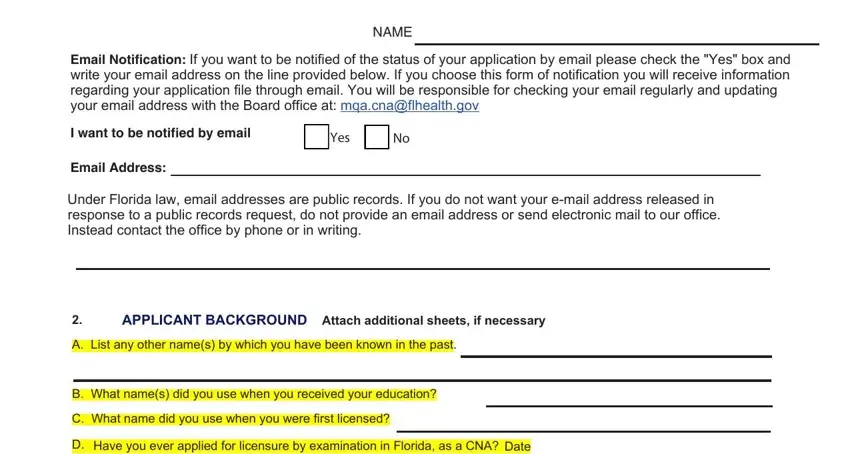
Describe the rights and responsibilities of the parties within the field Yes, Have you ever applied for, Date, Yes, F Have you ever been licensed in, Yes, Have you ever been denied or is, Yes, and If you answer Yes to question G in.
End by looking at the following areas and preparing them accordingly: H List all CNA licenses, active inactive or lapsed, NAME, StateCountry, License No, License Type, Date of Licensure, Status of License and Expiry Date, The Florida Board of Nursing, a state where you have a current, CRIMINAL HISTORY Answers to, Yes, and Have you EVER been convicted of or.
Step 3: Choose the Done button to save your form. So now it is at your disposal for transfer to your gadget.
Step 4: Come up with a copy of every different document. It would save you time and assist you to stay clear of complications in the long run. Also, your information is not revealed or viewed by us.
