It is easy to obtain documents making use of our PDF editor. Improving the cologuard referral form form is straightforward if you check out the following steps:
Step 1: Hit the orange "Get Form Now" button on the following website page.
Step 2: At this point, you may change your cologuard referral form. The multifunctional toolbar permits you to add, eliminate, modify, highlight, and also undertake many other commands to the text and areas inside the form.
If you want to prepare the template, type in the information the platform will require you to for each of the appropriate segments:
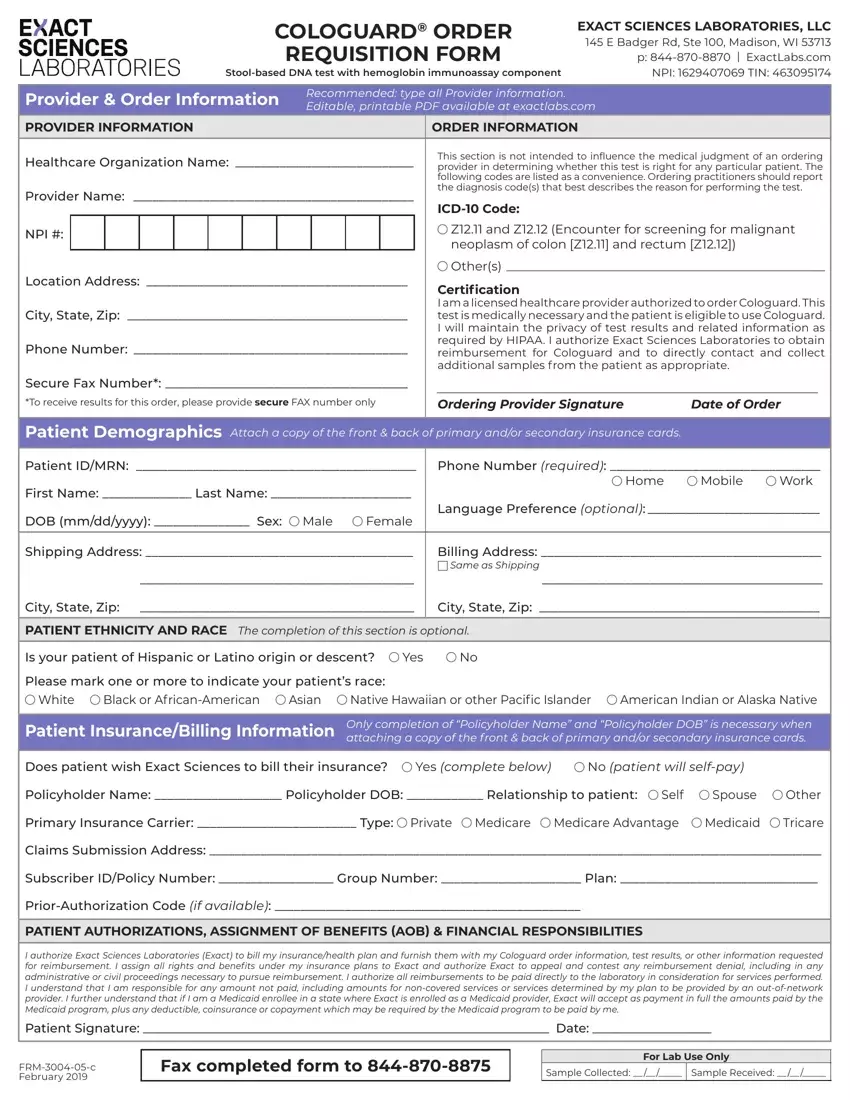
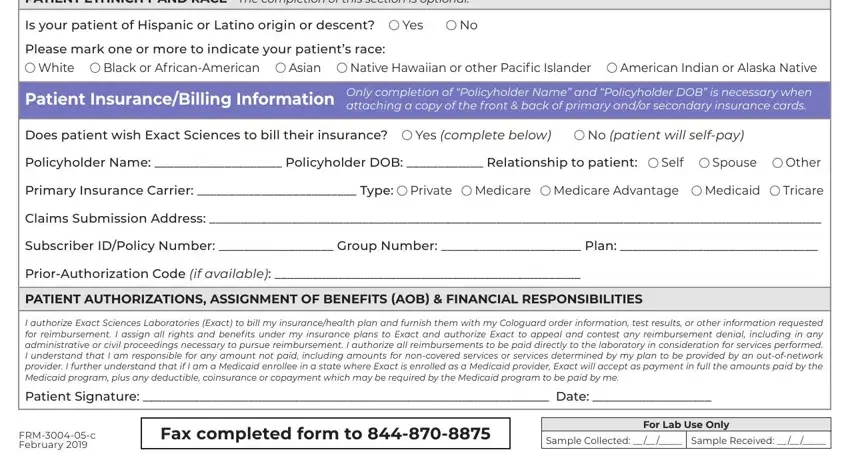
Fill in the PATIENT ETHNICITY AND RACE The, Is your patient of Hispanic or, Yes, Please mark one or more to, White, Black or AfricanAmerican, Asian, Native Hawaiian or other Pacific, American Indian or Alaska Native, Patient InsuranceBilling, Only completion of Policyholder, Does patient wish Exact Sciences, Yes complete below, No patient will selfpay, and Policyholder Name Policyholder areas with any data that will be requested by the program.
Step 3: Press the "Done" button. Now, you may export your PDF file - upload it to your electronic device or forward it through electronic mail.
Step 4: It's going to be more convenient to save duplicates of the form. You can rest assured that we won't display or read your details.
