
Our finest computer programmers have worked collectively to create the PDF editor you are going to benefit from. The following application allows you to create nc workers compensation form 18 documentation instantly and without problems. This is certainly everything you need to do.
Step 1: Choose the button "Get Form Here" on this site and hit it.
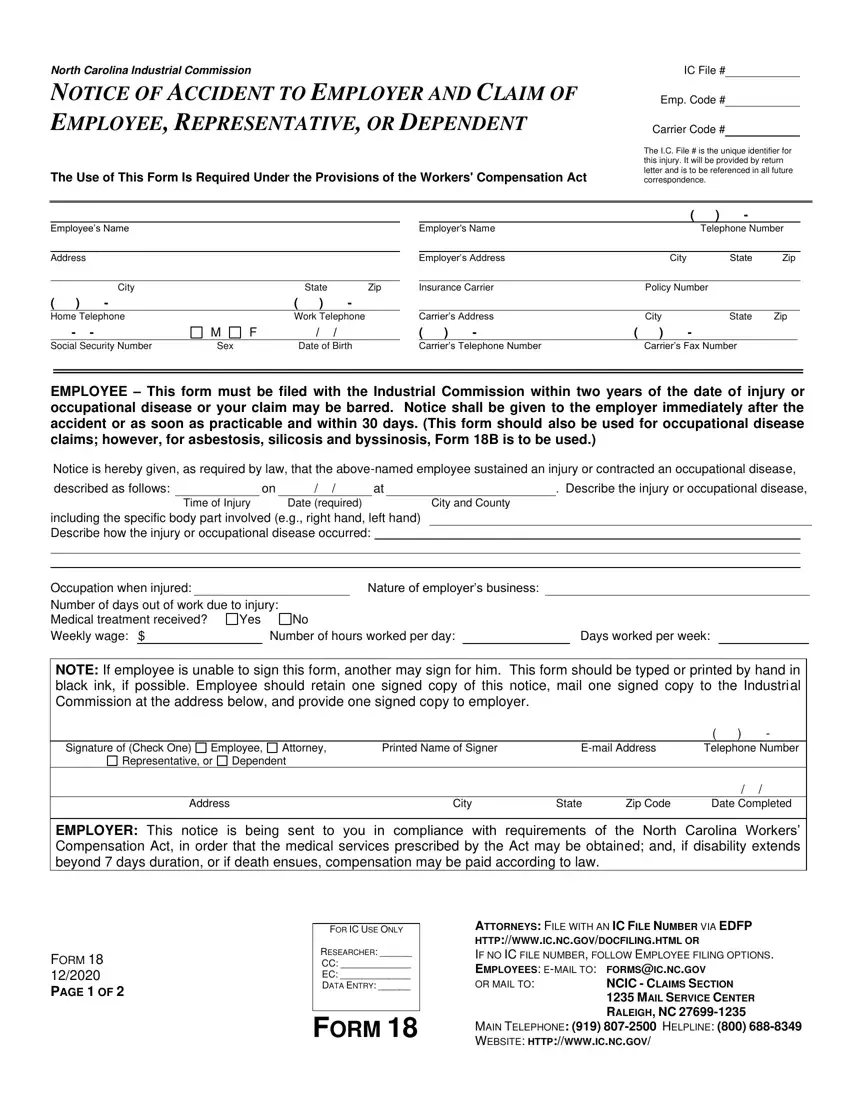
Step 2: You can now change the nc workers compensation form 18. You can use the multifunctional toolbar to add, erase, and change the content material of the form.
Enter the content demanded by the system to create the file.
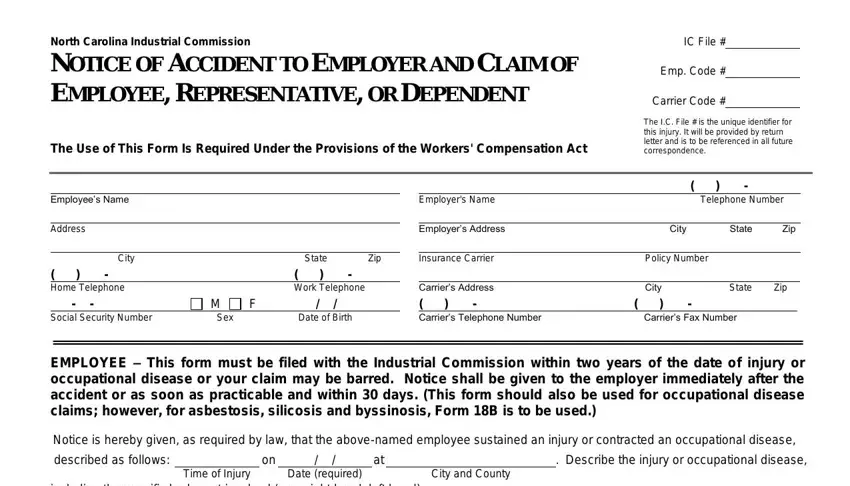
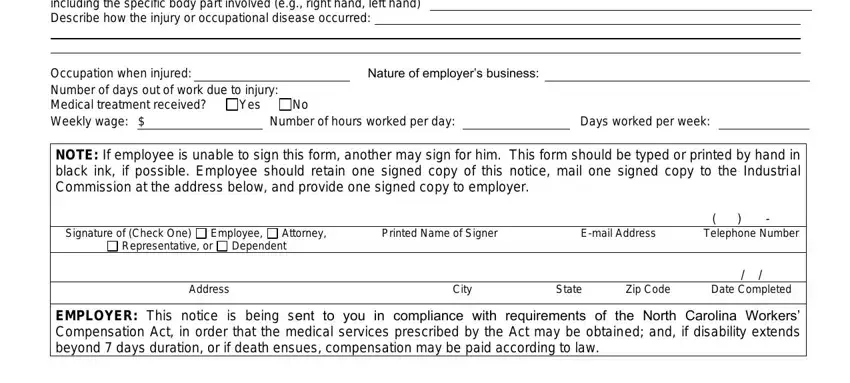
Type in the appropriate information in the field including the specific body part, Occupation when injured Number of, Nature of employers business, Number of hours worked per day, Days worked per week, NOTE If employee is unable to sign, Signature of Check One, Employee, Attorney, Printed Name of Signer, Email Address, Representative or, Dependent, Address, and City.
Step 3: Once you click the Done button, your prepared form can be easily transferred to each of your gadgets or to email chosen by you.
Step 4: Have a copy of every different file. It would save you some time and allow you to prevent worries in the future. Also, your information isn't used or analyzed by us.
