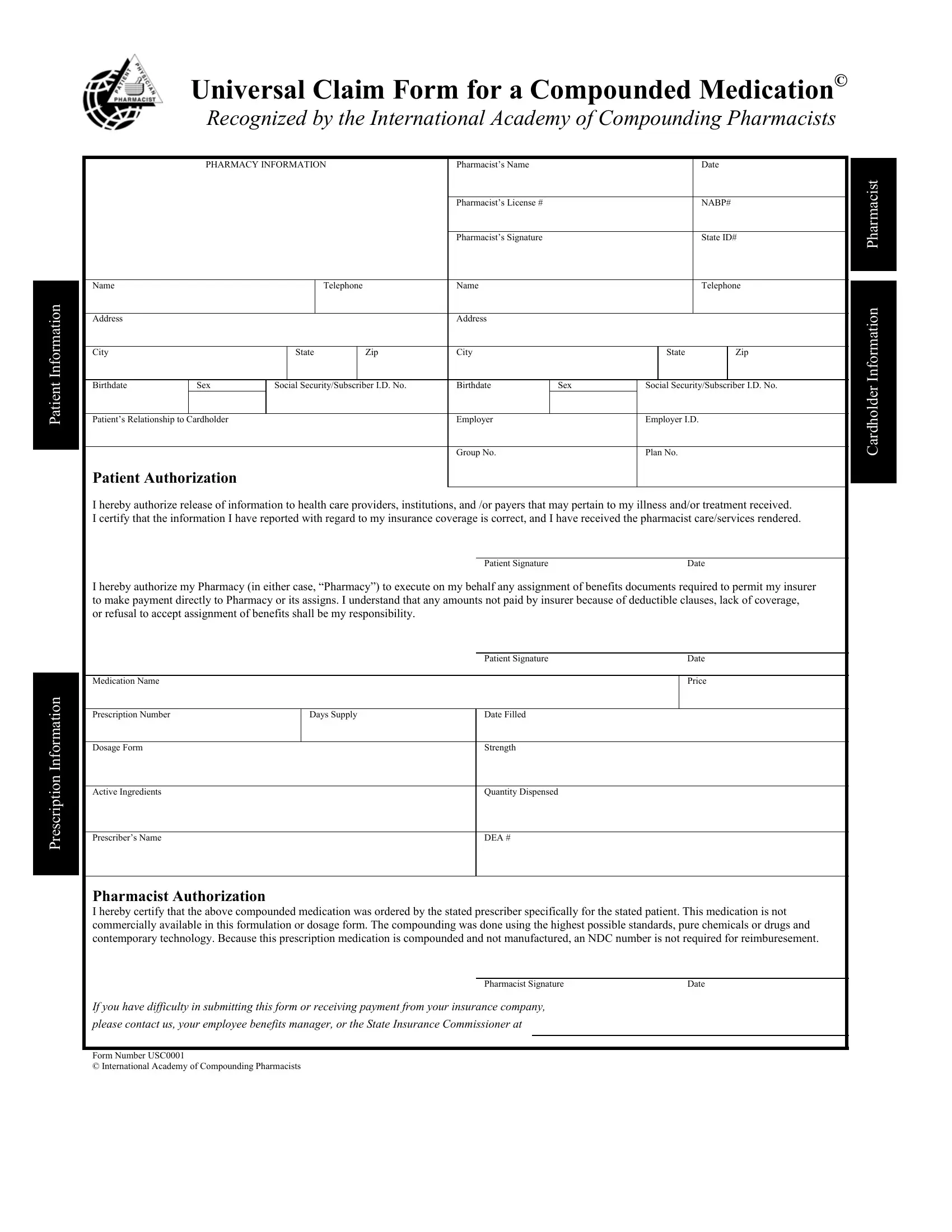
At first glance, navigating through healthcare paperwork can seem like a daunting task, but the Compounding Universal Claim Form offers a streamlined process for those needing to claim compounded medications. Developed with the expertise of the International Academy of Compounding Pharmacists, this form is a crucial tool for ensuring that patients, healthcare providers, and pharmacies communicate efficiently and effectively. It encompasses comprehensive sections for patient information, prescription details, and pharmacy identification, thus providing a thorough outline for the claims process. This includes capturing essential data such as patient demographics, prescription specifics, pharmacist credentials, and authorization for the release and receipt of medical information. Moreover, it addresses insurance aspects, by facilitating direct payment arrangements between insurers and pharmacies. Recognized and utilized universally, the form simplifies the submission and processing of claims related to compounded medications - a boon for those requiring special formulations that are not commercially available. Through this, the form not only aids in the financial aspects but also supports the delivery of personalized patient care, embodying a significant development in the healthcare field.
| Question | Answer |
|---|---|
| Form Name | Compounding Universal Claim Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | universal claim forms for compounded prescriptions, blank universal claim form for a compounded medication, universal claim form compounding, caremark compound prescription claim form |
Patient Information
Prescription Information
Universal Claim Form for a Compounded Medication©
Recognized by the International Academy of Compounding Pharmacists
|
PHARMACY INFORMATION |
|
Pharmacist’s Name |
|
|
|
|
Date |
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Pharmacist |
|
|
|
|
|
|
|
Pharmacist’s License # |
|
|
|
|
NABP# |
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Pharmacist’s Signature |
|
|
|
|
State ID# |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Name |
|
|
|
Telephone |
|
Name |
|
|
|
|
Telephone |
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Information |
Address |
|
|
|
|
|
|
Address |
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
City |
|
|
State |
|
Zip |
City |
|
|
State |
|
Zip |
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
||||
Birthdate |
Sex |
Social Security/Subscriber I.D. No. |
Birthdate |
Sex |
Social Security/Subscriber I.D. No. |
|
Cardholder |
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
Patient’s Relationship to Cardholder |
|
|
|
|
|
Group No. |
|
Plan No. |
|
|
|||||
|
|
|
|
|
Employer |
|
Employer I.D. |
|
|
|
|
||||
Patient Authorization
I hereby authorize release of information to health care providers, institutions, and /or payers that may pertain to my illness and/or treatment received. I certify that the information I have reported with regard to my insurance coverage is correct, and I have received the pharmacist care/services rendered.
Patient Signature |
Date |
I hereby authorize my Pharmacy (in either case, “Pharmacy”) to execute on my behalf any assignment of benefits documents required to permit my insurer to make payment directly to Pharmacy or its assigns. I understand that any amounts not paid by insurer because of deductible clauses, lack of coverage, or refusal to accept assignment of benefits shall be my responsibility.
|
|
Patient Signature |
Date |
|
|
|
|
Medication Name |
|
|
Price |
|
|
|
|
Prescription Number |
Days Supply |
Date Filled |
|
|
|
|
|
Dosage Form |
|
Strength |
|
|
|
|
|
Active Ingredients |
|
Quantity Dispensed |
|
|
|
|
|
Prescriber’s Name |
|
DEA # |
|
|
|
|
|
Pharmacist Authorization
I hereby certify that the above compounded medication was ordered by the stated prescriber specifically for the stated patient. This medication is not commercially available in this formulation or dosage form. The compounding was done using the highest possible standards, pure chemicals or drugs and contemporary technology. Because this prescription medication is compounded and not manufactured, an NDC number is not required for reimburesement.
Pharmacist Signature |
Date |
If you have difficulty in submitting this form or receiving payment from your insurance company,
please contact us, your employee benefits manager, or the State Insurance Commissioner at
Form Number USC0001
© International Academy of Compounding Pharmacists