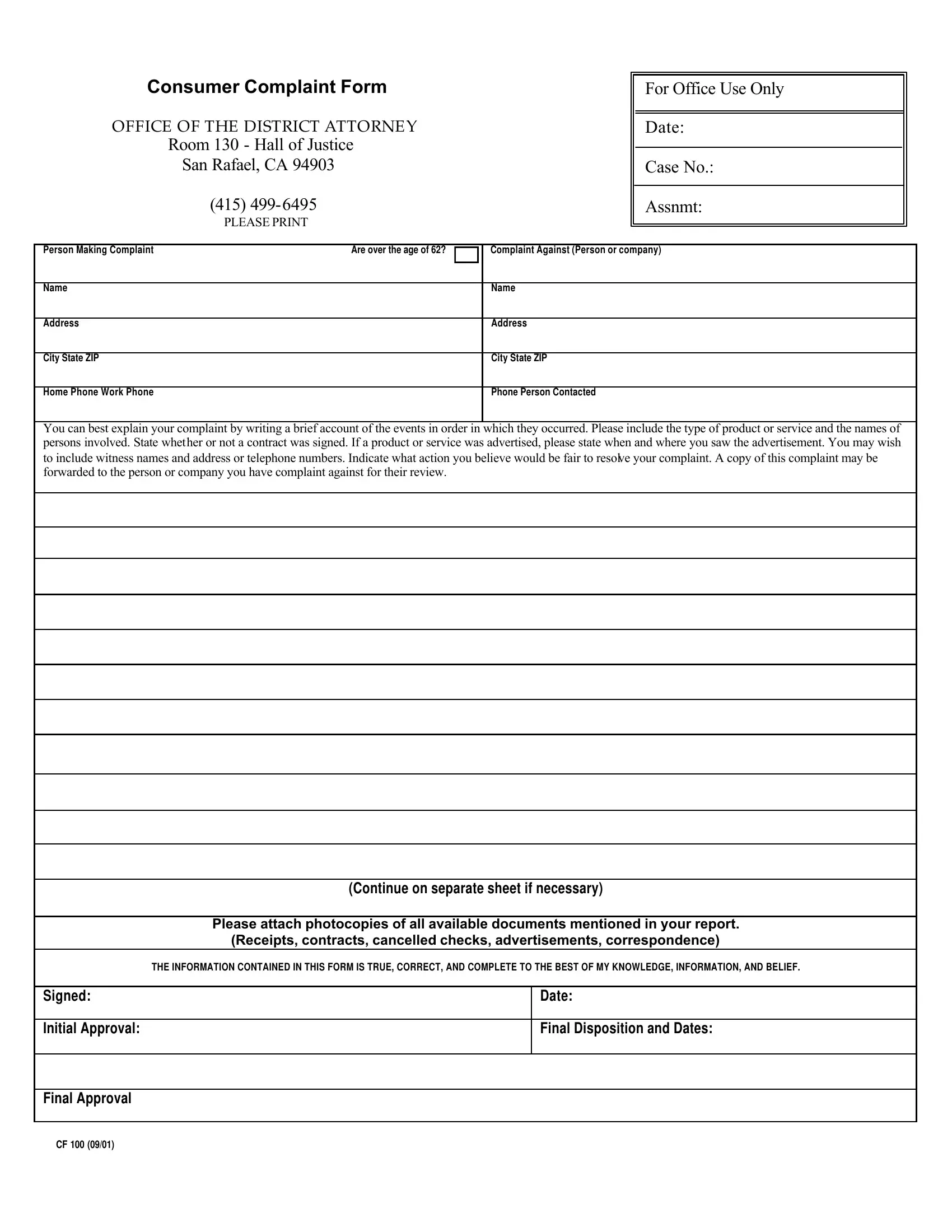
When individuals encounter problems with goods or services, they often feel powerless against corporations or businesses. However, the Consumer Complaint form, provided by the Office of the District Attorney in Marin County, serves as a crucial tool for those seeking justice and resolution. Intended to document grievances related to products or services accurately, this form requires complainants to provide detailed information about their issues, including a chronological account of events, the type of product or service involved, and details of any contracts signed or advertisements seen. Importantly, it also asks for suggested fair resolutions to the complaint, underscoring the complainant’s role in the mediation process. To substantiate claims, the form prompts for the attachment of relevant documents such as receipts, contracts, and correspondence. Furthermore, it includes a declaration by the complainant attesting to the truthfulness of the information provided, thereby laying the foundation for a potential legal or mediation process. Once completed and signed, this form is to be mailed to the Marin County District Attorney’s Consumer Protection Division, which not only mediates disputes but also enforces consumer protection laws, emphasizing the form's role in both dispute resolution and legal enforcement.
| Question | Answer |
|---|---|
| Form Name | Consumer Complaint Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | california form cf100, consumer complaint form, form cf 100 consumer, bbb complaint form pdf |
Consumer Complaint Form
OFFICE OF THE DISTRICT ATTORNE Y
Room 130 - Hall of Justice
San Rafael, CA 94903
(415)
PLEASE PRINT
For Office Use Only
Date:
Case No.:
Assnmt:
Person Making Complaint |
Are over the age of 62? |
Complaint Against (Person or company)
Name
Name
Address
Address
City State ZIP
City State ZIP
Home Phone Work Phone
Phone Person Contacted
You can best explain your complaint by writing a brief account of the events in order in which they occurred. Please include the type of product or service and the names of persons involved. State whether or not a contract was signed. If a product or service was advertised, please state when and where you saw the advertisement. You may wish to include witness names and address or telephone numbers. Indicate what action you believe would be fair to resolve your complaint. A copy of this complaint may be forwarded to the person or company you have complaint against for their review.
(Continue on separate sheet if necessary)
Please attach photocopies of all available documents mentioned in your report. (Receipts, contracts, cancelled checks, advertisements, correspondence)
THE INFORMATION CONTAINED IN THIS FORM IS TRUE, CORRECT, AND COMPLETE TO THE BEST OF MY KNOWLEDGE, INFORMATION, AND BELIEF.
Signed:
Initial Approval:
Date:
Final Disposition and Dates:
Final Approval
CF 100 (09/01)
The Consumer Protection Division of the Marin County District Attorney’s Office provides mediation for consumer complaints and enforces consumer protection laws.
1)FILL OUT the form
2)ATTACH any photocopies of all available documents mentioned in your report. (Receipts, contracts, cancelled checks, advertisements, correspondence)
3)SIGN the form
4)MAIL the form TO:
Office of the District Attorney
Consumer Protection
3501 Civic Center Dr.
Hall of Justice, Room 130
San Rafael, Ca. 94903