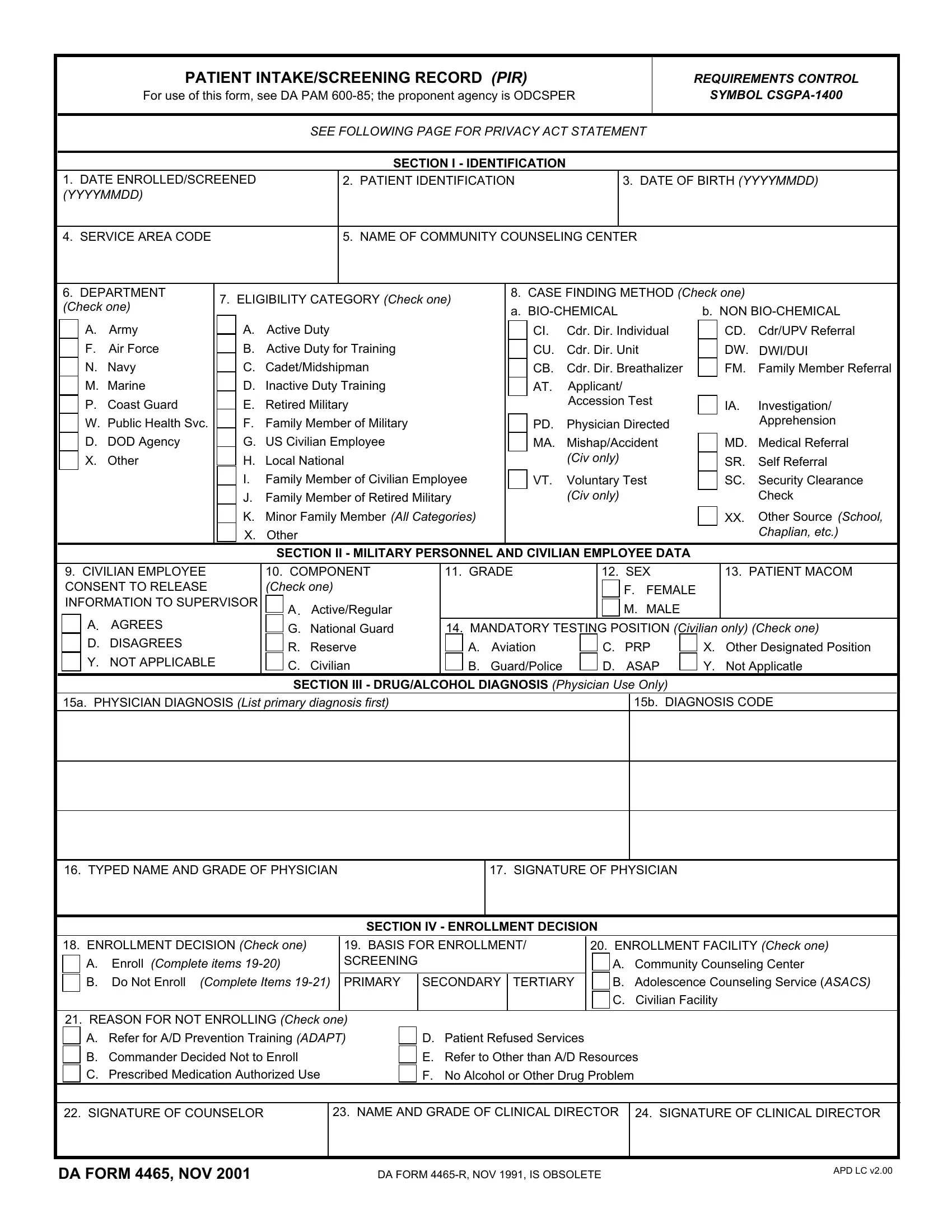
The DA 4465 Patient Intake/Screening Record (PIR) is the primary administrative document used during Army Substance Abuse Program (ASAP) enrollment. It is governed by DA PAM 600-85 under the Office of the Deputy Chief of Staff for Personnel (ODCSPER).
The form collects data in five key areas. The first area covers patient identification: full name, date of birth, DoD ID number, grade, and unit assignment. The second area records the eligibility category, which is one of four types: active duty soldier, National Guard or Reserve member, DoD civilian employee, or eligible family member. The third area documents the case finding method, such as self-referral, command referral, medical referral, or a positive urinalysis result.
The fourth area is the clinical diagnosis section. A licensed physician or mental health clinician enters the substance-related diagnosis using DSM-5 or ICD-10 codes. The diagnosis category, which is abuse, dependence, or non-dependent use, maps to a specific ASAP treatment track. The fifth area records the enrollment decision, including the date and counselor signature.
For active duty soldiers, completing the form is mandatory. Civilian DoD employees and family members who voluntarily seek ASAP services also complete it. A Privacy Act Statement on the form outlines how personal health information is used, who may access it, and what the disclosure rules are for each eligibility category.
The PIR supports individualized treatment planning, command accountability reporting, and DoD-wide substance abuse program data collection across all Army installations worldwide.
| Question | Answer |
|---|---|
| Form Name | Da Form 4465 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | patient screening record pir, patient pir form, pir armypubs fillable, da 4465 form |