
How to Fill Out DA Form 5018 R Online
Follow these steps to complete DA Form 5018 R using FormsPal's free PDF editor:
- Open the form. Click the Fill Out Form button to launch the fillable DA Form 5018 R in your browser.
- Enter client information. Add your full name, unit, and Social Security Number in Section A.
- Name the authorized recipient. Specify the individual or organization authorized to receive your treatment information.
- Select information type. Check the boxes for each type of information to be released: diagnosis, prognosis, treatment details, or rehabilitation progress.
- Set expiration terms. Enter the date or event on which your consent expires, as required by Section B.
- Sign and date. Read the consent statement carefully, then add your signature and the date of signing.
- Download or print. Save the completed form as a PDF or print it for submission to your commanding officer.
Key Sections of the DA Form 5018 R
The form has three sections, each with a distinct purpose:
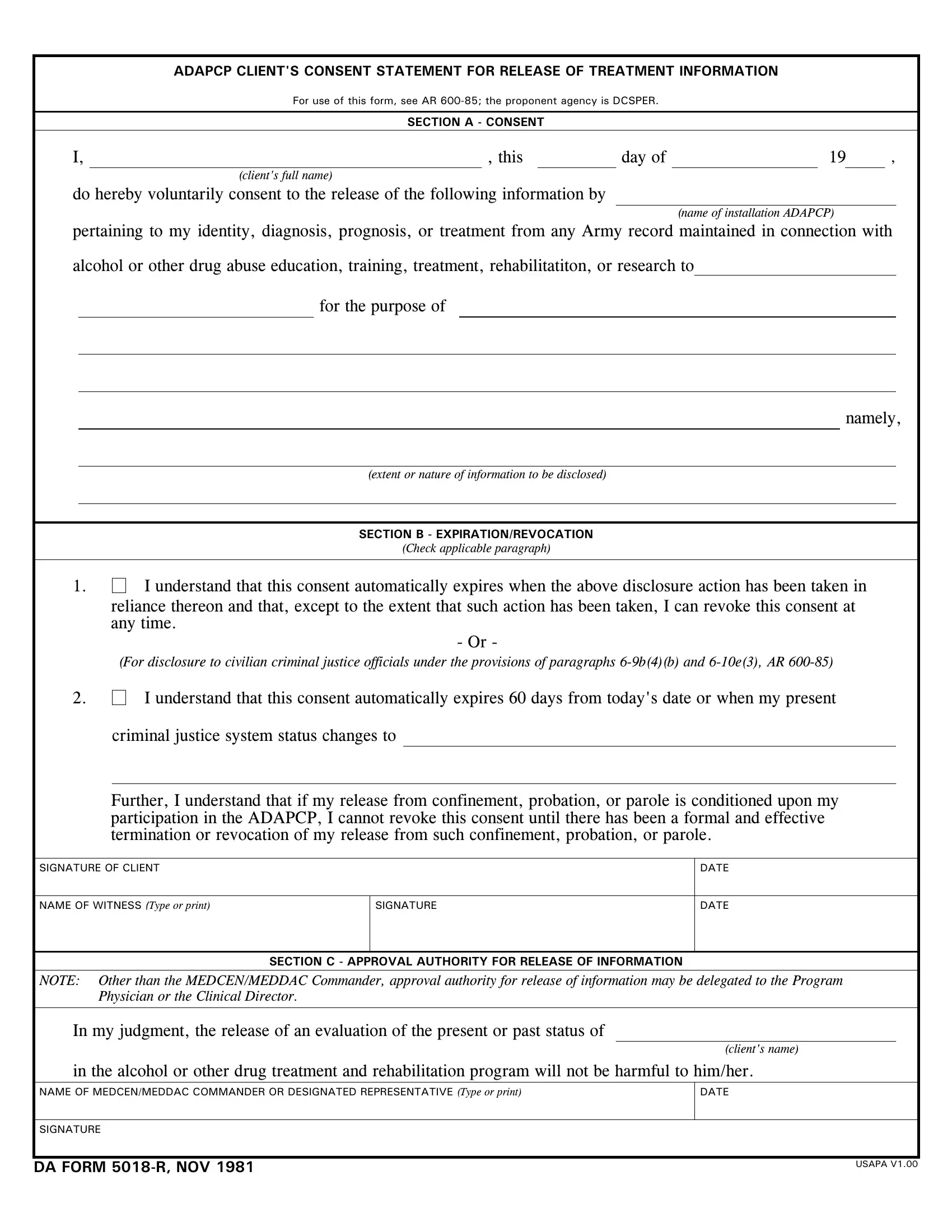
- Section A - Consent Statement. Records the client's voluntary agreement to release named treatment information to specified parties.
- Section B - Expiration and Revocation. Defines the consent expiration date and outlines the client's right to revoke consent at any time before that date.
- Section C - Approval Authority. Requires an authorized official to confirm that the disclosure does not harm the client before any information is shared.
When to Complete DA Form 5018 R
Soldiers file the DA Form 5018 R when they need to share ADAPCP treatment records with approved parties. Common situations include coordination between Army medical personnel and civilian healthcare providers, transfers between Army units that require treatment continuity, and legal proceedings involving civilian criminal justice officials.
Related Army and Medical Consent Forms
After completing the DA Form 5018 R, you may also need the DA Form 5019-R for related ADAPCP program requirements. Soldiers managing general medical records may use the Medical Management Authorization Form. For substance abuse program documentation, see the Drug Testing Consent Form.