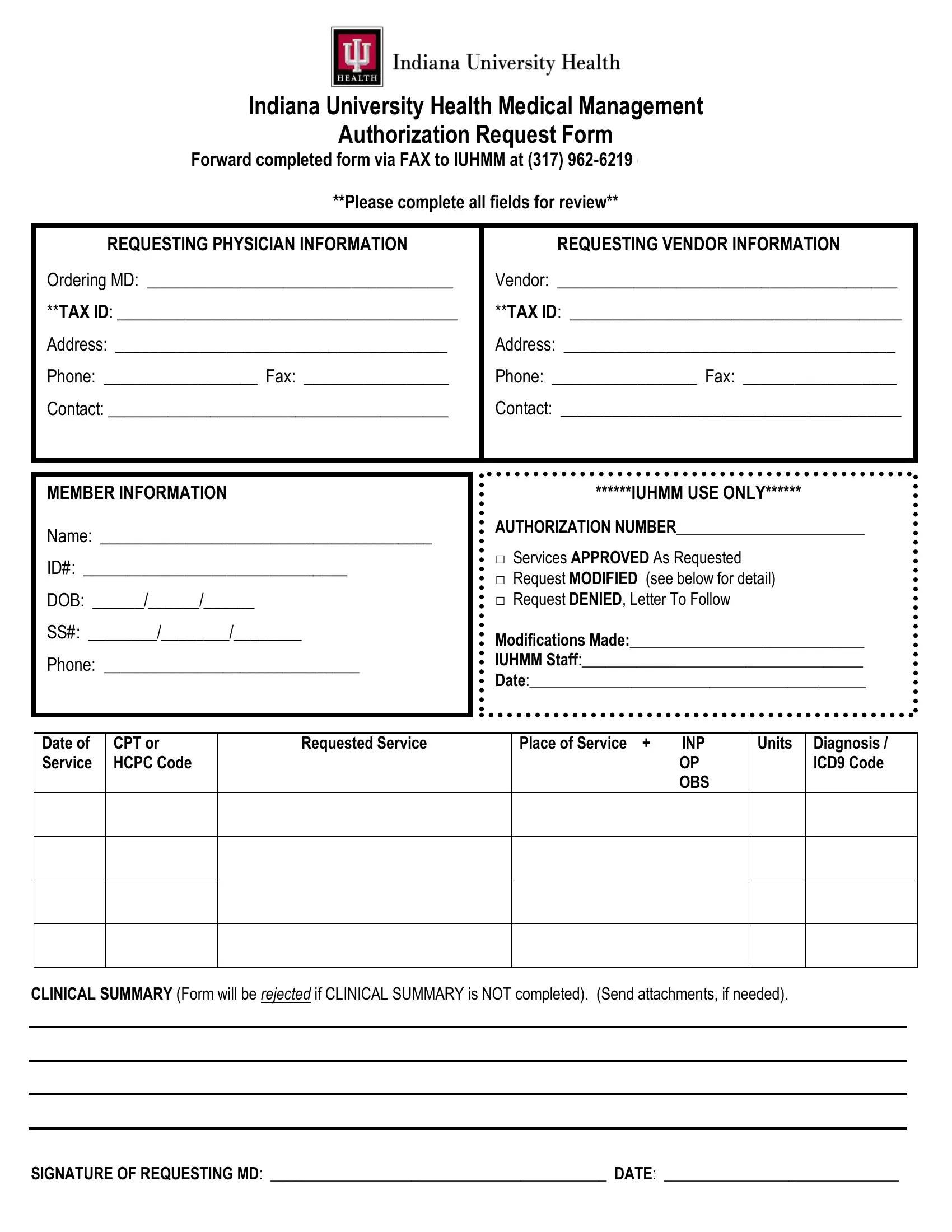
In the realm of healthcare, the coordination and authorization of medical services are pivotal to ensuring that patients receive the timely and appropriate care they need. The Indiana University Health Medical Management Authorization Request Form is a critical instrument in this process, serving as a bridge between healthcare providers, insurance entities, and patients. This comprehensive form requires detailed information from the requesting physician and vendor, including Tax IDs, contact details, and a concise clinical summary of the patient's condition. The form meticulously captures member information, including name, identification number, date of birth, and contact details, ensuring that the patient's identity and needs are clearly communicated. Crucially, this form also features a section for the medical management team's use only, where authorization decisions are recorded—marking whether services have been approved, modified, or denied. This document not only facilitates the efficient processing of requests but also plays a significant role in transparency and accountability in the healthcare system. By completing all fields and providing a clinical summary, healthcare providers can expedite the review process and move one step closer to securing the necessary services for their patients.
| Question | Answer |
|---|---|
| Form Name | Medical Management Authorization Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | medical management authorization, indiana health request form, indiana medical request form, id information iuhmm form |
Indiana University Health Medical Management
Authorization Request Form
Forward completed form via FAX to IUHMM at (317)
**Please complete all fields for review**
REQUESTING PHYSICIAN INFORMATION |
REQUESTING VENDOR INFORMATION |
Ordering MD: ____________________________________ |
Vendor: ________________________________________ |
**TAX ID: ________________________________________ |
**TAX ID: _______________________________________ |
Address: _______________________________________ |
Address: _______________________________________ |
Phone: __________________ Fax: _________________ |
Phone: _________________ Fax: __________________ |
Contact: ________________________________________ |
Contact: ________________________________________ |
|
|
MEMBER INFORMATION
Name: _______________________________________
ID#: _______________________________
DOB: ______/______/______
SS#: ________/________/________
Phone: ______________________________
******IUHMM USE ONLY******
AUTHORIZATION NUMBER________________________
□Services APPROVED As Requested
□Request MODIFIED (see below for detail)
□Request DENIED, Letter To Follow
Modifications Made:______________________________
IUHMM Staff:____________________________________
Date:___________________________________________
Date of Service
CPT or HCPC Code
Requested Service
Place of Service + |
INP |
|
OP |
|
OBS |
Units
Diagnosis / ICD9 Code
CLINICAL SUMMARY (Form will be rejected if CLINICAL SUMMARY is NOT completed). (Send attachments, if needed).
SIGNATURE OF REQUESTING MD: ___________________________________________ DATE: ______________________________