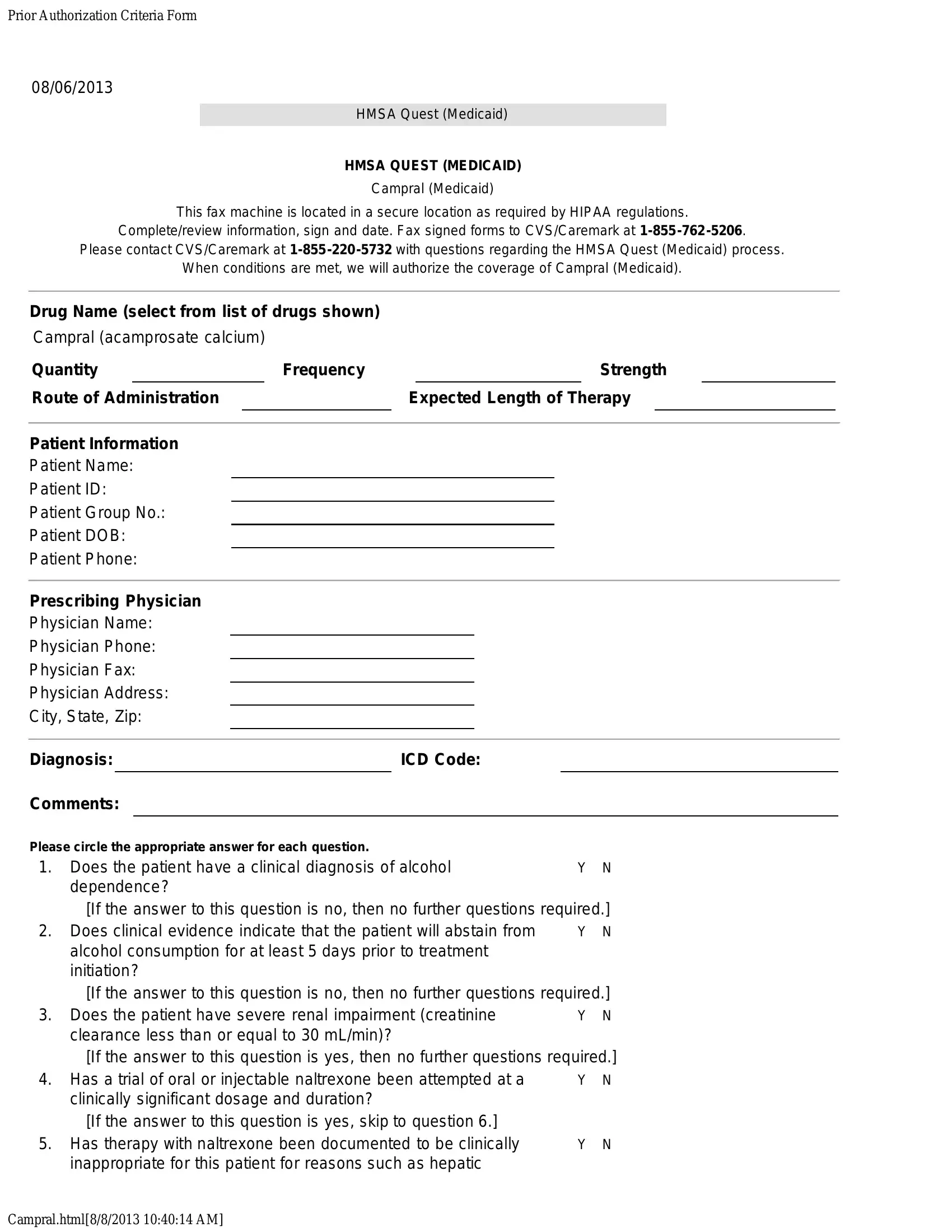
The HMSA Quest Prior Authorization form serves as a critical tool in the process of obtaining coverage for specific medications under the HMSA Quest (Medicaid) program, with explicit focus on the medication Campral (acamprosate calcium). Created to ensure that medications are used in a safe, effective, and appropriate manner, this document requires detailed information about the patient’s condition, as well as the medication requested. Dated August 6, 2013, the form adheres to strict HIPAA regulations to maintain patient confidentiality, mandating that it be completed, signed, and then faxed to CVS/Caremark for processing. It embodies a series of criteria that need to be met before authorization for coverage can be granted, including clinical diagnosis, previous treatment attempts, and the planned duration of therapy. Questions designed to assess the appropriateness of Campral based on prior alcohol dependence treatment, potential renal impairment, and the inclusion in a broader psychosocial treatment program highlight the form’s comprehensive approach to evaluating treatment necessity and efficacy. With specific instructions for direct communication with CVS/Caremark for questions regarding the process, it exemplifies a streamlined mechanism aimed at ensuring that patients receive the most suitable medication support within the framework of Medicaid provisions.
| Question | Answer |
|---|---|
| Form Name | HMSA Quest Prior Authorization Form |
| Form Length | 1 pages |
| Fillable? | Yes |
| Fillable fields | 72 |
| Avg. time to fill out | 14 min 43 sec |
| Other names | hmsa quest prior authorization medication, mavenclad prior authorization criteria, hmsaq quest pa drug, empire blue cross blue shield pdf prior auth request forms |