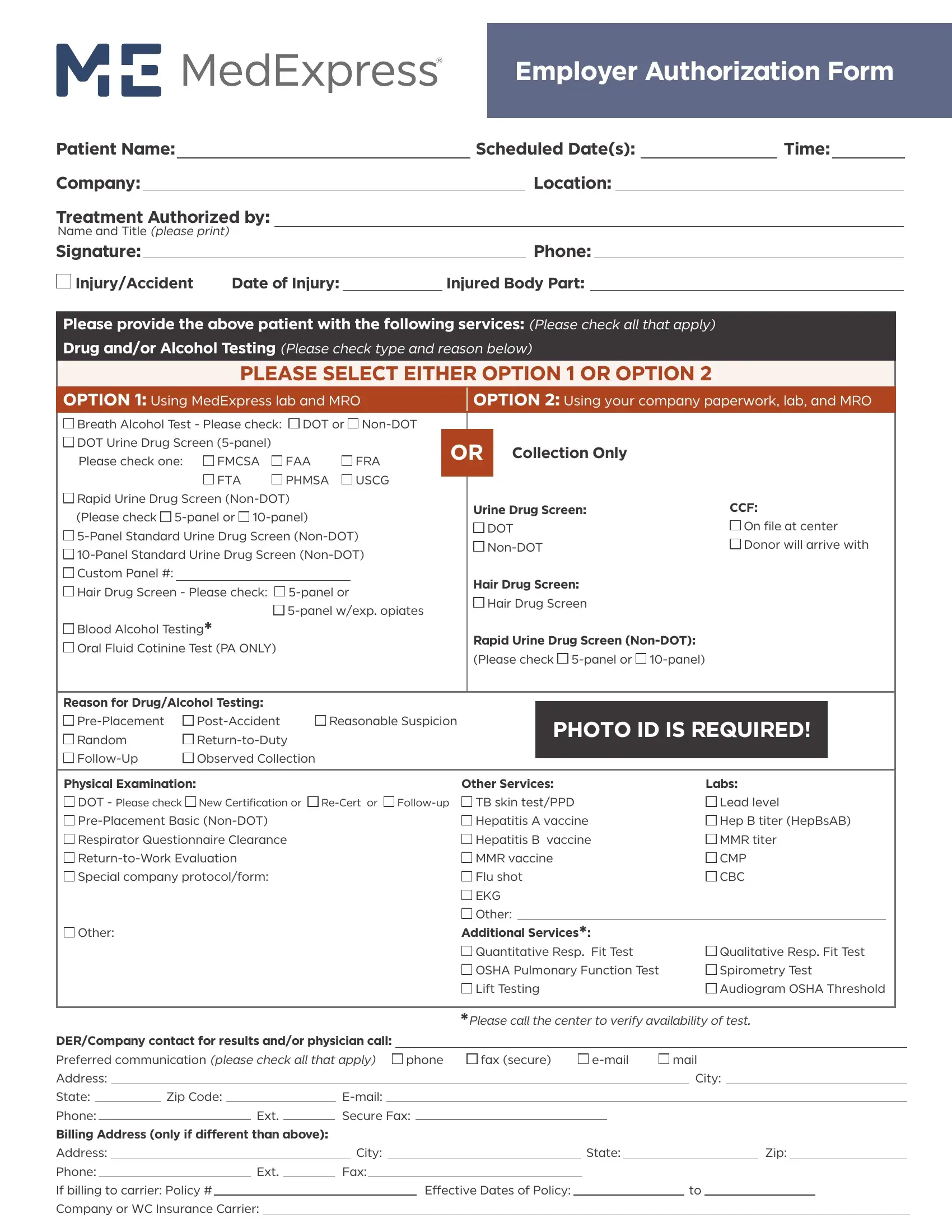
At the core of workplace safety and compliance, the MedExpress Employer Authorization Form serves a pivotal role. This detailed form, meticulously designed, allows employers to authorize medical services for their employees, ranging from drug and alcohol testing to physical examinations and specialized services like respiratory fit tests and audiograms. The form requires basic patient information, including the patient's name, the scheduled date and time for the service, and the company's details. It also necessitates a thorough specification of the treatment authorized, encompassing a wide array of checks like DOT and non-DOT drug screenings, breath alcohol tests, and custom panel drug screens. Additionally, the form offers options for using MedExpress's lab and Medical Review Officer (MRO) or the company's own paperwork and lab services for processing. Moreover, specific to the instances necessitating these tests—such as pre-placement, post-accident, or for reasonable suspicion among others—the form ensures clarity and precision. Instructions are included for the collection of specimens, like urine or hair for drug screening, and the necessity for photo ID at the time of the test. Fees around physical examinations and other medical services like vaccinations, titers, and evaluations for return to work are also addressed, ensuring employers have a comprehensive tool for employee health and safety management. Furthermore, the form facilitates communication preferences for the delivery of results and specifies the billing address, if different from the primary address, demonstrating its all-encompassing nature in managing occupational health processes efficiently and effectively.
| Question | Answer |
|---|---|
| Form Name | Medexpress Employer Authorization Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | med express employeer auth forms, authorization form medexpress, employer authorization med express, med express employer authorization form has no confirmation number |