
In case you desire to fill out authorizations, you don't need to download any sort of programs - just give a try to our online PDF editor. To make our tool better and simpler to work with, we consistently work on new features, with our users' suggestions in mind. Getting underway is simple! All you have to do is take the following basic steps below:
Step 1: Simply click on the "Get Form Button" above on this webpage to get into our form editor. There you will find everything that is necessary to work with your file.
Step 2: The editor offers you the opportunity to work with almost all PDF files in many different ways. Change it with your own text, correct original content, and put in a signature - all readily available!
It will be simple to complete the pdf using this detailed guide! Here's what you should do:
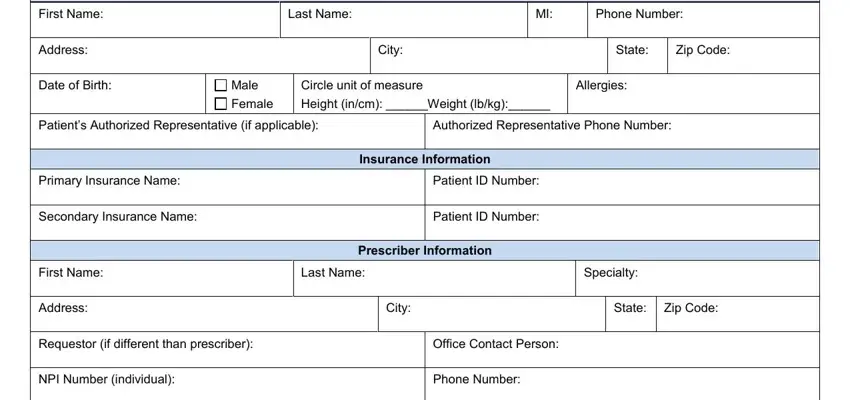
1. You will want to fill out the authorizations accurately, therefore take care when filling in the parts including these blank fields:
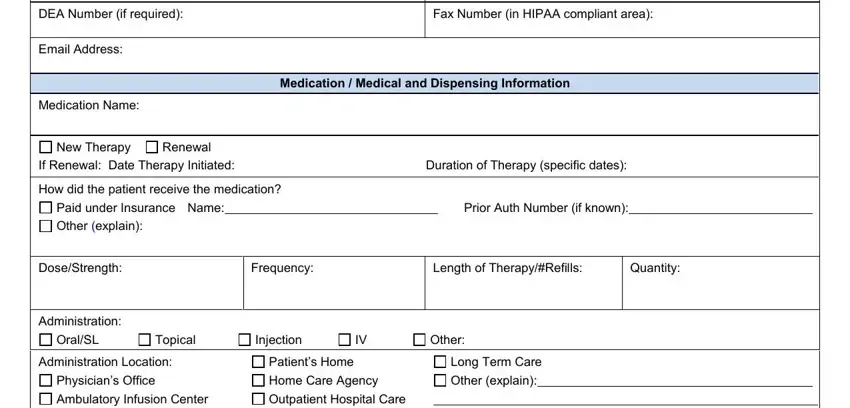
2. When this array of fields is done, you need to put in the necessary specifics in DEA Number if required, Fax Number in HIPAA compliant area, Email Address, Medication Name, New Therapy, Renewal, Medication Medical and Dispensing, If Renewal Date Therapy Initiated, How did the patient receive the, Paid under Insurance Name, Prior Auth Number if known, Other explain, DoseStrength, Frequency, and Length of TherapyRefills in order to move on further.
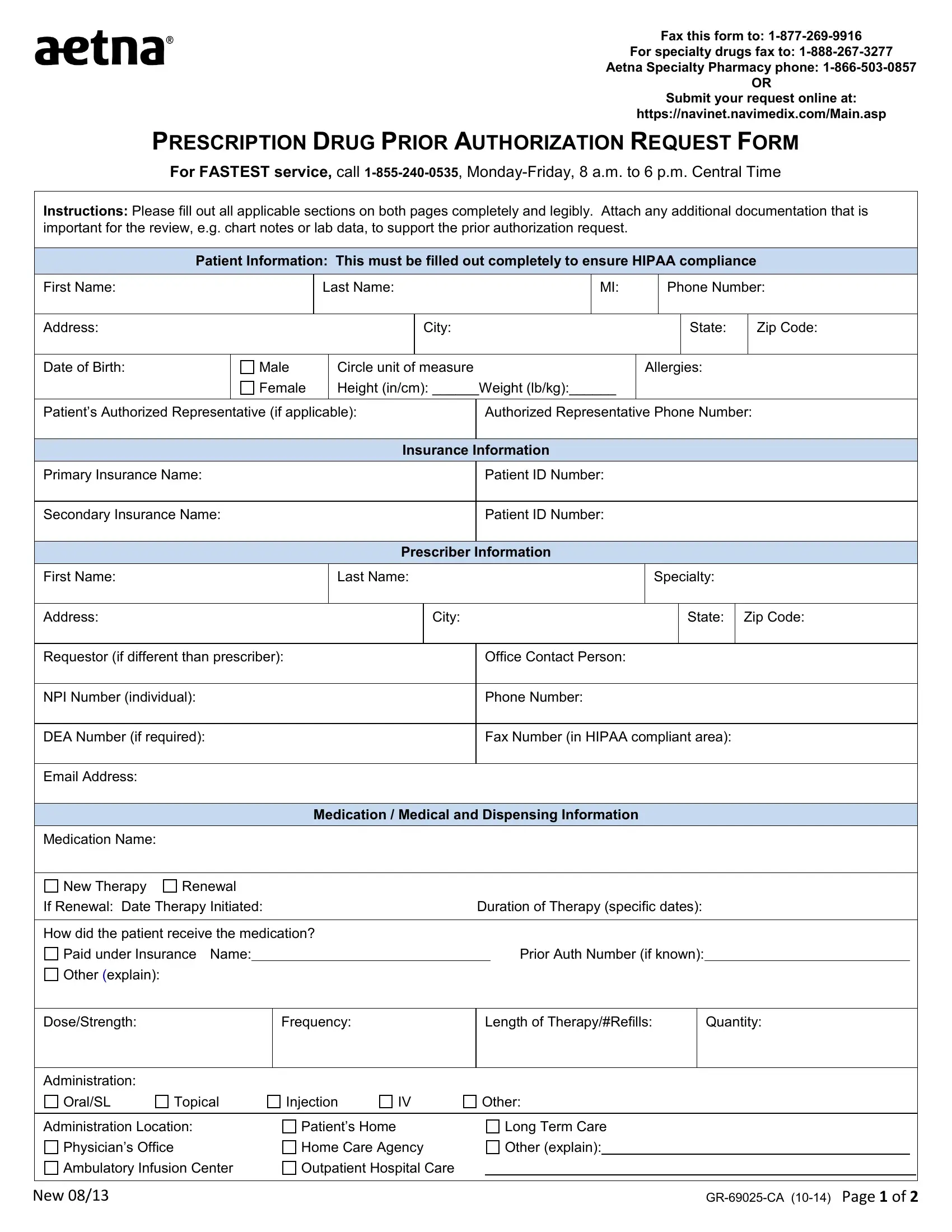
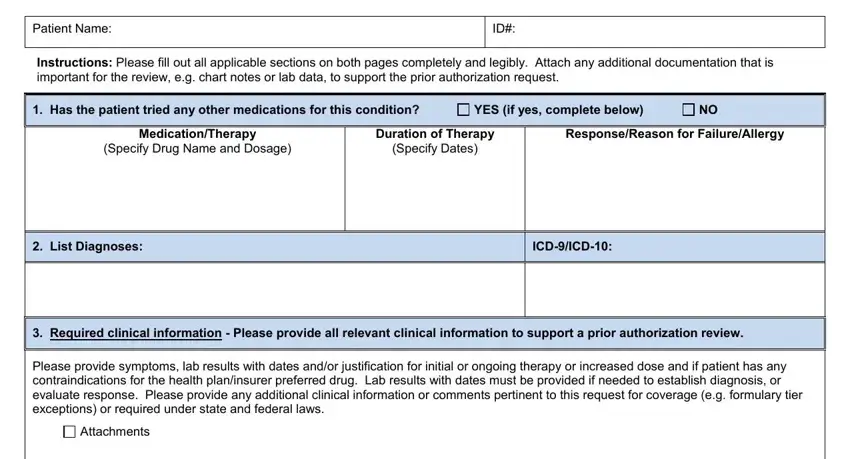
3. This next part is focused on PRESCRIPTION DRUG PRIOR, Patient Name, Instructions Please fill out all, Has the patient tried any other, YES if yes complete below, MedicationTherapy, Specify Drug Name and Dosage, Duration of Therapy, Specify Dates, ResponseReason for FailureAllergy, List Diagnoses, ICDICD, Required clinical information, Please provide symptoms lab, and Attachments - fill out these blanks.
4. Your next subsection needs your involvement in the following places: Attestation I attest the, Prescriber Signature, Date, Confidentiality Notice The, Plan Use Only, Date of Decision, Approved, Denied CommentsInformation, and New. Be sure that you give all needed information to move forward.
Be very careful when filling in New and Plan Use Only, since this is the section where a lot of people make a few mistakes.
Step 3: After you've reviewed the details you given, click on "Done" to finalize your form at FormsPal. Find your authorizations once you sign up for a free trial. Conveniently view the form within your personal account, with any edits and changes being automatically saved! FormsPal is dedicated to the privacy of our users; we always make sure that all personal information processed by our system continues to be confidential.