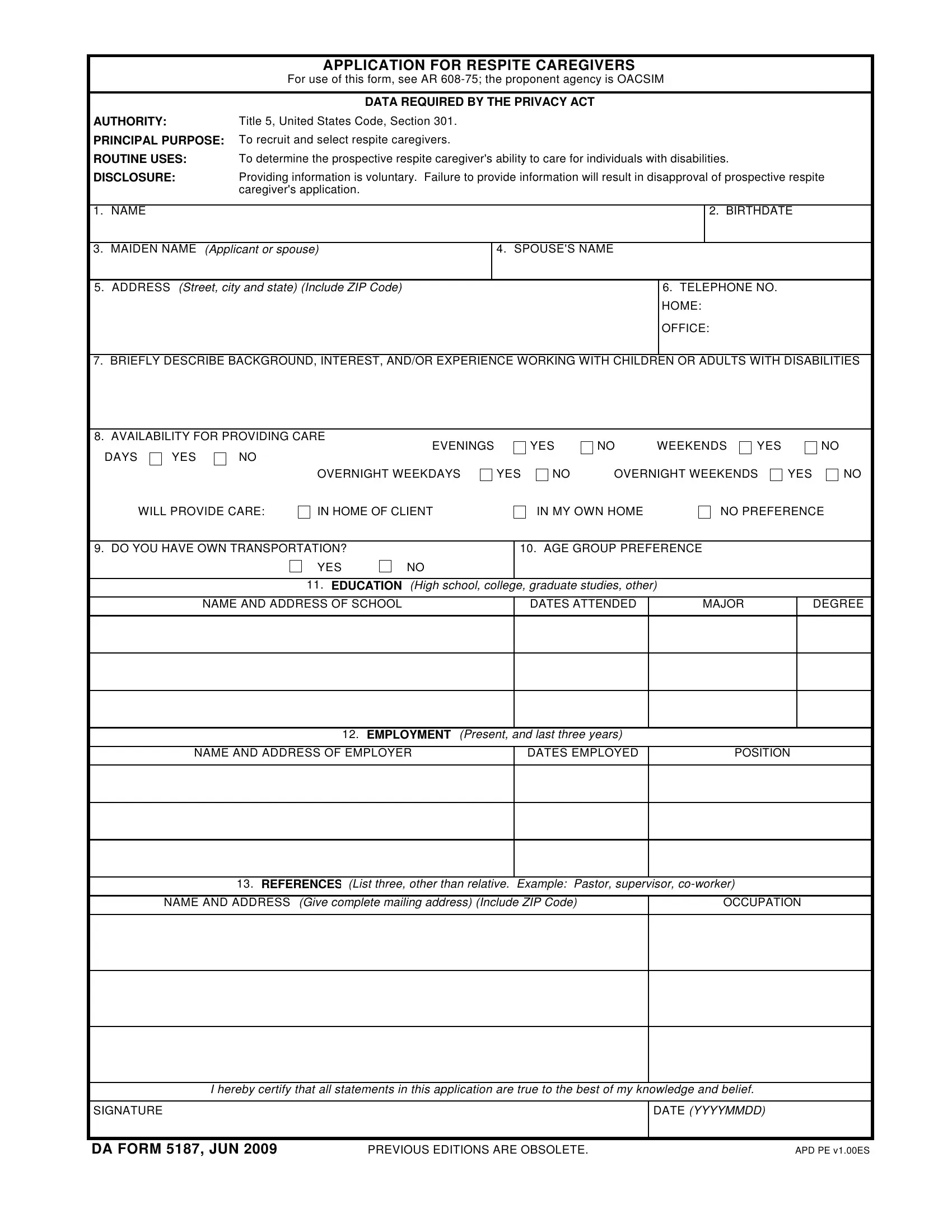
In the realm of support and care for individuals with disabilities, the role of a respite caregiver stands as a lighthouse of relief for families navigating through the stormy waters of daily care needs. At the heart of the recruitment and selection process for these critical roles lies the DA Form 5187, an official document designed under the guidelines specified in AR 608-75 by the Office of the Assistant Chief of Staff for Installation Management (OACSIM). This form serves as the bridge between potential caregivers and the opportunity to make a significant difference in the lives of individuals with disabilities. It meticulously gathers essential information, ranging from personal identification to educational background, employment history, and specific preferences in terms of care provision, such as availability and age groups preferred to work with. By submitting this form, applicants not only express their willingness to fulfill this noble role but also align themselves with the legal and procedural frameworks that ensure the highest standards of care are met. Moreover, the DA Form 5187 underscores the importance of transparency and honesty by requiring applicants to certify the truthfulness of their provided information, embedding a layer of trust from the onset. In essence, this form does not merely filter candidates; it lays the cornerstone for a compassionate and comprehensive caregivers’ network, dedicated to enhancing the quality of life for individuals with disabilities.
| Question | Answer |
|---|---|
| Form Name | Da Form 5187 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | 00ES, amazon, CAREGIVERS, RESPITE |
|
APPLICATION FOR RESPITE CAREGIVERS |
|
|
For use of this form, see AR |
|
|
|
|
|
DATA REQUIRED BY THE PRIVACY ACT |
|
AUTHORITY: |
Title 5, United States Code, Section 301. |
|
PRINCIPAL PURPOSE: |
To recruit and select respite caregivers. |
|
ROUTINE USES: |
To determine the prospective respite caregiver's ability to care for individuals with disabilities. |
|
DISCLOSURE: |
Providing information is voluntary. Failure to provide information will result in disapproval of prospective respite |
|
|
caregiver's application. |
|
|
|
|
1. NAME |
|
2. BIRTHDATE |
|
|
|
3. MAIDEN NAME (Applicant or spouse)
4. SPOUSE'S NAME
5. ADDRESS (Street, city and state) (Include ZIP Code)
6.TELEPHONE NO. HOME:
OFFICE:
7. BRIEFLY DESCRIBE BACKGROUND, INTEREST, AND/OR EXPERIENCE WORKING WITH CHILDREN OR ADULTS WITH DISABILITIES
8. AVAILABILITY FOR PROVIDING CARE
EVENINGS
DAYS YES NO
YES
NOWEEKENDS
YES
NO
WILL PROVIDE CARE:
OVERNIGHT WEEKDAYS
IN HOME OF CLIENT
YES
NO |
OVERNIGHT WEEKENDS |
YES |
|
IN MY OWN HOME |
NO PREFERENCE |
||
NO
9. DO YOU HAVE OWN TRANSPORTATION? |
|
10. AGE GROUP PREFERENCE |
YES |
NO |
|
|
|
|
11. EDUCATION (High school, college, graduate studies, other)
NAME AND ADDRESS OF SCHOOL
DATES ATTENDED
MAJOR
DEGREE
12. EMPLOYMENT (Present, and last three years)
NAME AND ADDRESS OF EMPLOYER
DATES EMPLOYED
POSITION
13. REFERENCES (List three, other than relative. Example: Pastor, supervisor,
NAME AND ADDRESS (Give complete mailing address) (Include ZIP Code)
OCCUPATION
I hereby certify that all statements in this application are true to the best of my knowledge and belief.
SIGNATURE |
DATE (YYYYMMDD) |
|
|
DA FORM 5187, JUN 2009 |
PREVIOUS EDITIONS ARE OBSOLETE. |
APD PE v1.00ES |