
5888 form can be completed effortlessly. Just try FormsPal PDF editing tool to perform the job quickly. To make our editor better and more convenient to use, we constantly work on new features, with our users' suggestions in mind. It merely requires a couple of simple steps:
Step 1: First, access the pdf tool by pressing the "Get Form Button" above on this page.
Step 2: This tool grants the capability to modify PDF forms in various ways. Modify it by adding any text, adjust what's originally in the document, and put in a signature - all at your convenience!
As for the blank fields of this specific document, this is what you want to do:
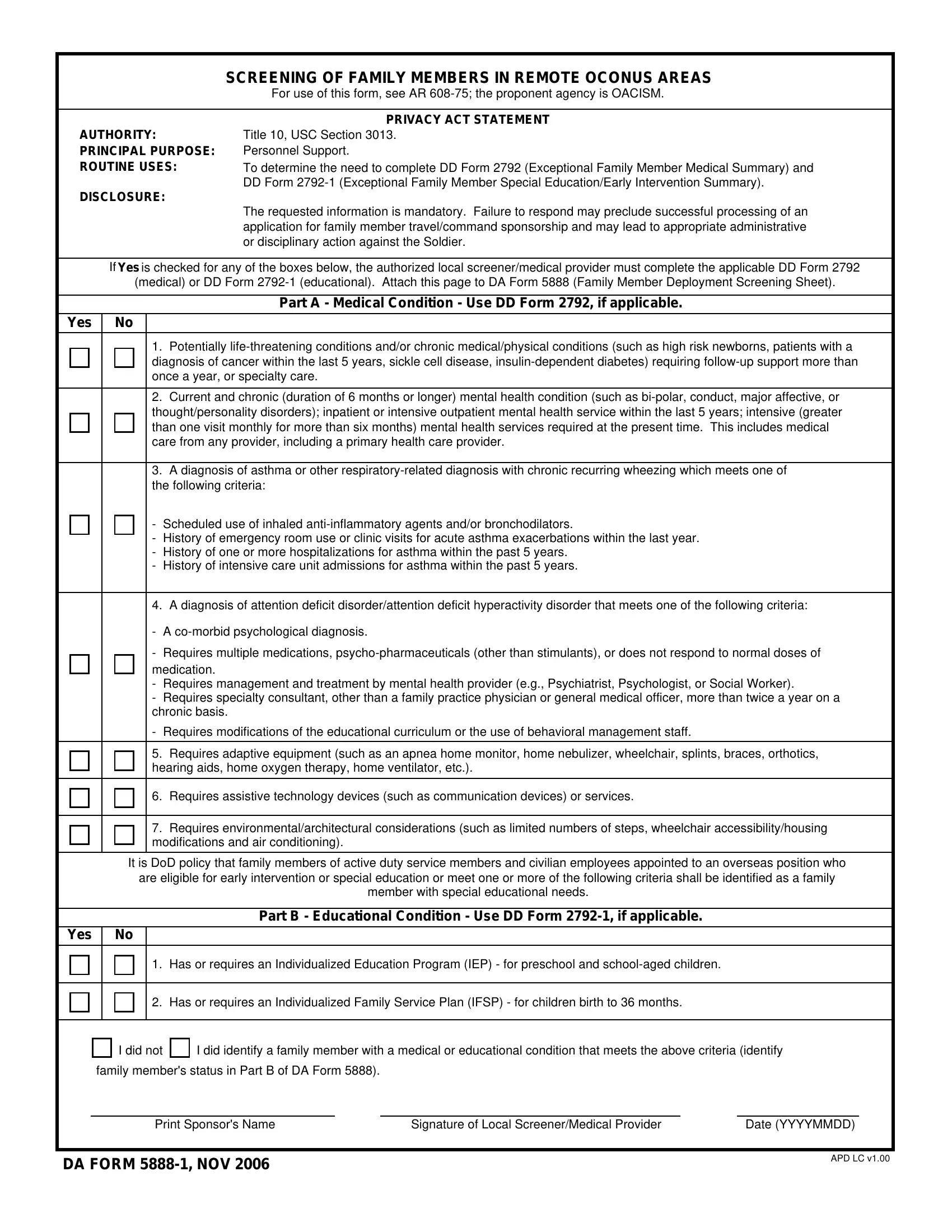
1. Whenever filling out the 5888 form, be sure to incorporate all needed blank fields in their corresponding area. This will help to hasten the work, making it possible for your information to be handled efficiently and properly.
2. Once the last array of blanks is completed, go on to type in the suitable information in all these: Requires adaptive equipment such, Requires assistive technology, Requires, It is DoD policy that family, are eligible for early, member with special educational, Part B Educational Condition Use, Yes, Has or requires an Individualized, Has or requires an Individualized, I did not, I did identify a family member, family members status in Part B of, Print Sponsors Name, and Signature of Local ScreenerMedical.
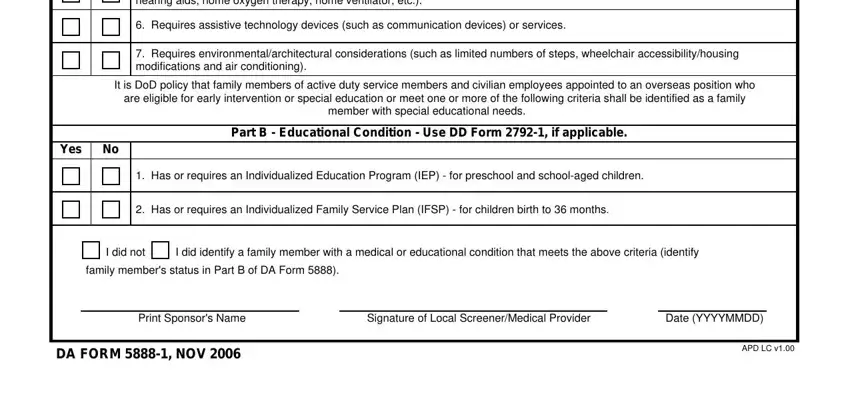
Always be very careful while filling out I did identify a family member and family members status in Part B of, as this is the part in which most people make a few mistakes.
Step 3: Prior to getting to the next step, make sure that all form fields are filled in the correct way. As soon as you confirm that it is good, click on “Done." Sign up with us today and instantly get access to 5888 form, ready for download. All alterations you make are saved , making it possible to modify the pdf at a later time as needed. Whenever you work with FormsPal, you're able to fill out documents without the need to worry about personal information leaks or entries getting shared. Our protected platform ensures that your private details are kept safe.