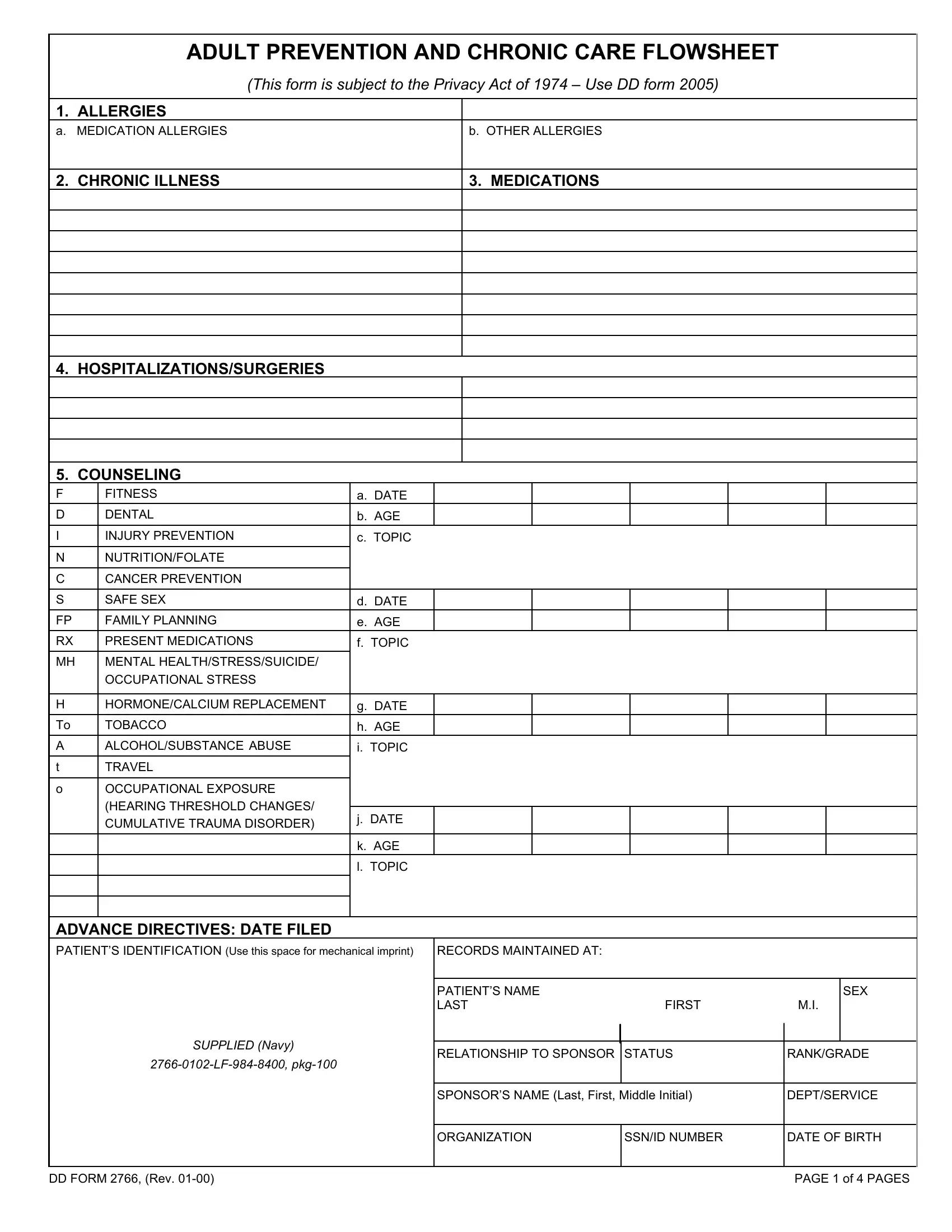
In the structured framework of military health records, the DD Form 2766, also known as the Adult Prevention and Chronic Care Flowsheet, stands out as a comprehensive document designed for meticulous recording of an individual's health history within the armed forces. Rooted in the Privacy Act of 1974, this form ensures the protection of personal health information, offering sections for detailed accounts of allergies, both to medications and other sources, and chronic illnesses, which are critical for ongoing medical care and emergency situations. It catalogues medications, hospitalizations, surgeries, and counseling for fitness, encompassing a broad array of preventive measures and healthcare interventions. Its emphasis on counseling topics, such as nutrition, cancer prevention, safe sex, and mental health among others, highlights the military's commitment to holistic wellness. Furthermore, the form provides space for recording the patient's Identification details, including the pivotal Sponsor’s information, enhancing its utility in managing and retrieving medical records efficiently. Individuals' family medical history, crucial for understanding genetic risks, is thoroughly noted, alongside a comprehensive listing of screenings and exams relevant to prevention and early detection of diseases. Immunizations status, a critical component for readiness and preventing disease outbreak in enclosed military environments, is meticulously tracked. The form also delves into readiness checks, including DNA, blood type, and other health markers essential for deployment. Additionally, pre and post-deployment health statuses are captured, acknowledging the unique exposures and health risks associated with various deployment locations. The DD Form 2766 not only serves as a vital tool for individual healthcare management but also underscores the military's dedication to preserving the health and readiness of its personnel through preventive care and detailed health monitoring.
| Question | Answer |
|---|---|
| Form Name | DD 2766 Army Form |
| Form Length | 4 pages |
| Fillable? | Yes |
| Fillable fields | 555 |
| Avg. time to fill out | 37 min 20 sec |
| Other names | dd form 2766c vaccine administration record, dd 2766 army, dd 2766c, dd form 2766c |
ADULT PREVENTION AND CHRONIC CARE FLOWSHEET
(This form is subject to the Privacy Act of 1974 – Use DD form 2005)
1. ALLERGIES
a. MEDICATION ALLERGIES |
b. OTHER ALLERGIES |
2. CHRONIC ILLNESS
3. MEDICATIONS
4.HOSPITALIZATIONS/SURGERIES
5.COUNSELING
F |
FITNESS |
a. DATE |
|
|
|
|
|
D |
DENTAL |
b. AGE |
|
|
|
|
|
|
|
|
|
|
|
|
|
I |
INJURY PREVENTION |
c. TOPIC |
|||||
NNUTRITION/FOLATE
C CANCER PREVENTION
S |
SAFE SEX |
d. DATE |
|
|
|
|
|
FP |
FAMILY PLANNING |
e. AGE |
|
|
|
|
|
RX |
PRESENT MEDICATIONS |
f. TOPIC |
|||||
MH |
MENTAL HEALTH/STRESS/SUICIDE/ |
|
|
|
|
|
|
|
OCCUPATIONAL STRESS |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
H |
HORMONE/CALCIUM REPLACEMENT |
g. DATE |
|
|
|
|
|
To |
TOBACCO |
h. AGE |
|
|
|
|
|
A |
ALCOHOL/SUBSTANCE ABUSE |
i. TOPIC |
|||||
tTRAVEL
o |
OCCUPATIONAL EXPOSURE |
|
|
|
|
|
|
|
(HEARING THRESHOLD CHANGES/ |
|
|
|
|
|
|
|
j. DATE |
|
|
|
|
|
|
|
CUMULATIVE TRAUMA DISORDER) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
k. AGE |
|
|
|
|
|
|
|
l. TOPIC |
|||||
ADVANCE DIRECTIVES: DATE FILED
PATIENT’S IDENTIFICATION (Use this space for mechanical imprint) RECORDS MAINTAINED AT:
|
PATIENT’S NAME |
|
|
SEX |
|
|
LAST |
FIRST |
M.I. |
|
|
SUPPLIED (Navy) |
|
|
|
|
|
|
|
|
|
||
RELATIONSHIP TO SPONSOR |
STATUS |
RANK/GRADE |
|||
|
|
|
|
||
|
|
|
|
||
|
SPONSOR’S NAME (Last, First, Middle Initial) |
DEPT/SERVICE |
|||
|
|
|
|
||
|
ORGANIZATION |
SSN/ID NUMBER |
DATE OF BIRTH |
||
|
|
|
|
|
|
DD FORM 2766, (Rev. |
PAGE 1 of 4 PAGES |
ADULT PREVENTION AND CHRONIC CARE FLOWSHEET
6.FAMILY HISTORY M = Mother, F = Father, S = Sibling, MGM = Maternal Grandmother, MGF – Maternal Grandfather, PGM = Paternal Grandmother, PGF = Paternal Grandfather)
a. CANCER (Specify)
b.CARDIOVASCULAR DISEASE (Specify)
c.DIABETES (Specify)
d.MENTAL ILLNESS/CHEMICAL DEPENDENCY (Specify)
7.SCREENING EXAMS (* = Actual Result, ** = Tricare Benefit, N = Normal, X = Abnormal, E = Done Elsewhere, R = Refused, NA = Not Indicated) (● = Next Due)
|
a. TEST |
b. FREQUENCY |
c. YEAR |
|
|
|
|
|
|
|
d. AGE |
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(1) CLINICAL DISEASE |
ANNUAL |
|
|
|
e. DATES |
||||
PREV EVAL/PHA (HEAR) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
*(2) WEIGHT |
ANNUAL FOR ACTIVE DUTY |
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
||
*(3) HEIGHT |
ANNUAL FOR ACTIVE DUTY |
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
*(4) BLOOD PRESSURE |
ONCE q 2 YRS FOR BP < |
|
|
|
|
|
|
|
|
|
|
130/85, ANNUAL IF GREATER |
|
|
|
|
|
|
|
*(5) CHOLESTEROL** |
*q 5 YRS FOR AGE > 18 |
|
|
|
|
|
|
|
|
|
|
q YR IF PREV ABN |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(6) HEARING |
CLINICAL DISCRETION |
|
|
|
|
|
|
|
|
(7) SKIN EXAM (Cancer) |
ANNUAL IF AT RISK |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(8) ORAL/DENTAL ** |
ANNUAL |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ROUTINE ACUITY WITH PERIODIC |
|
|
|
|
|
|
|
(9) EYE/VISION** |
ASSESSMENT DIABETES ANNUAL |
|
|
|
|
|
|
||
GLAUCOMA CHECK: |
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
Blacks q |
|
|
|
|
|
|
|
|
|
All q |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(10) |
BREAST EXAM |
ANNUAL: > 40 YRS |
|
|
|
|
|
|
|
(11) |
MAMMOGRAM** |
BASELINE @ 40, q 2 YRS |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
BASELINE: AGE 18 OR ONSET OF |
|
|
|
|
|
|
|
(12) |
PAP |
SEXUAL ACTIVITY |
|
|
|
|
|
|
|
**(Digital Rectal Exam) |
AFTER 3 NL ANNUAL EXAMS, |
|
|
|
|
|
|
||
PERFORM q |
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(13) |
FECAL OCCULT |
ANNUAL > 50 yrs |
|
|
|
|
|
|
|
BLOOD |
|
|
|
|
|
|
|
|
|
(14) |
SIGMOID |
EVERY |
|
|
|
|
|
|
|
(15) |
COLONOSCOPY |
HIGH RISK q 5 YRS > 40 YRS |
|
|
|
|
|
|
|
(16) |
TESTICULAR |
HIGH RISK ANNUAL |
|
|
|
|
|
|
|
(17) |
PROSTATE** |
WITH P.E. > 40 YRS (Presently |
|
|
|
|
|
|
|
**(DIGITAL RECTAL EXAM) |
recommended annually) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(18) |
RUBELLA SCREEN |
ONCE BETWEEN AGES |
|
|
|
|
|
|
|
|
(Females) |
(Unless prev vaccinated) |
|
|
|
|
|
|
|
(19) |
OCCUPATIONAL |
APPROPRIATE TO EXPOSURES |
|
|
|
|
|
|
|
|
SCREENING EXAMS |
|
|
|
|
|
|
|
|
(20) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(21) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(22) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DD FORM 2766, (Rev. |
|
|
|
|
|
|
PAGE 2 of 4 PAGES |
||