
 TRAVEL ALLOWANCE
TRAVEL ALLOWANCE


 APPROVED
APPROVED 
 DISAPPROVED
DISAPPROVED



 SEPARATED
SEPARATED DIVORCED
DIVORCED

 YES
YES
 NO
NO
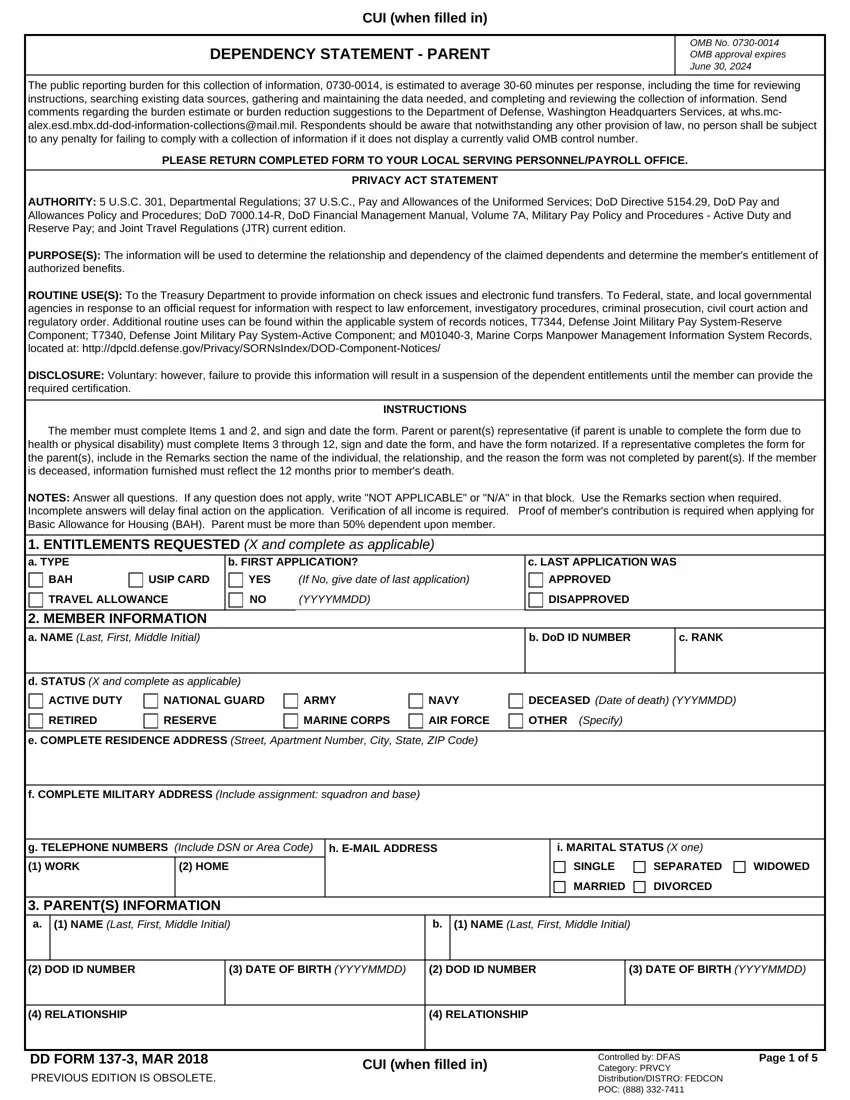
Handful of things can be quicker than preparing files making use of this PDF editor. There is not much you need to do to update the dd form 137 parent form - only follow these steps in the next order:
Step 1: To start out, click the orange button "Get Form Now".
Step 2: You're now able to change dd form 137 parent. You possess a variety of options with our multifunctional toolbar - you can include, remove, or customize the content material, highlight the certain elements, as well as undertake similar commands.
The next sections will make up the PDF document that you will be filling in:
Put the asked details in the RELATIONSHIP, RELATIONSHIP, DD FORM MAR PREVIOUS EDITION IS, CUI when filled in, Controlled by DFAS Category PRVCY, and Page of part.

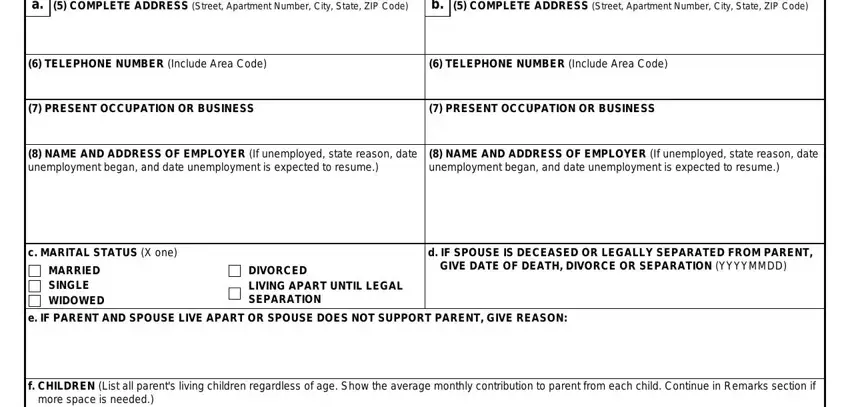
Put down all data you may need in the space PARENTS INFORMATION Continued a, COMPLETE ADDRESS Street Apartment, COMPLETE ADDRESS Street Apartment, TELEPHONE NUMBER Include Area Code, TELEPHONE NUMBER Include Area Code, PRESENT OCCUPATION OR BUSINESS, PRESENT OCCUPATION OR BUSINESS, NAME AND ADDRESS OF EMPLOYER If, NAME AND ADDRESS OF EMPLOYER If, c MARITAL STATUS X one, MARRIED SINGLE WIDOWED, DIVORCED LIVING APART UNTIL LEGAL, d IF SPOUSE IS DECEASED OR LEGALLY, GIVE DATE OF DEATH DIVORCE OR, and e IF PARENT AND SPOUSE LIVE APART.
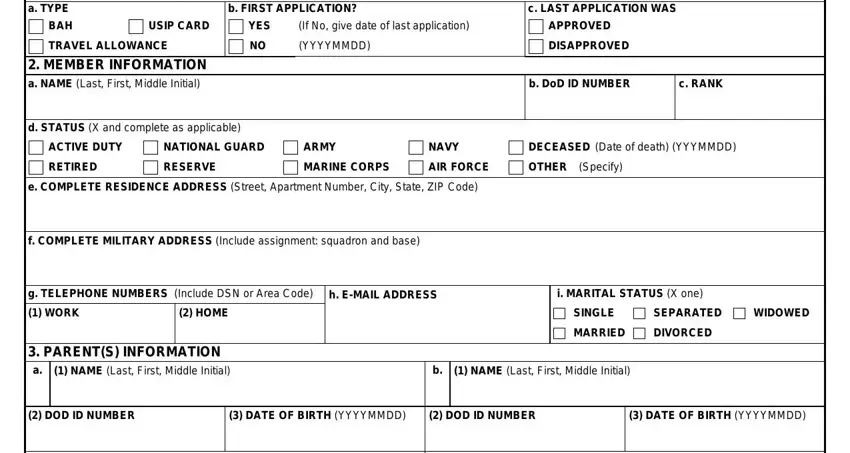
The area NAME Last First Middle Initial, DOD ID NUMBER Service Members Only, BRANCH OF SERVICE If on Active, MONTHLY CONTRIBUTION TO PARENT, g DOES ANY OTHER CHILD CLAIM, YES, PARENTS RESIDENCE a TYPE OF, HOME OR APARTMENT OF PARENT, HOME OR APARTMENT OF MEMBER Date, HOME OR APARTMENT OF FRIEND OR, HOSPITAL OR INSTITUTION, and OTHER Explain should be for you to insert each side's rights and obligations.
Finalize by looking at the following sections and completing them as required: b OWNER OF RESIDENCE, NAME Last First Middle Initial, ADDRESS Street Apartment Number, c IS RESIDENCE, SUBSIDIZED HOUSING, d DATE PARENT STARTED LIVING AT, YES, DD FORM MAR PREVIOUS EDITION IS, e IS CURRENT ADDRESS PARENTS, If No explain where else parent, YES, CUI when filled in, and Page of.

Step 3: When you choose the Done button, your finalized file can be easily transferred to any of your devices or to electronic mail stated by you.
Step 4: Create duplicates of the form - it can help you stay clear of forthcoming difficulties. And don't be concerned - we are not meant to distribute or see your information.
