
Any time you wish to fill out FRV, there's no need to install any sort of software - just try our online tool. To retain our editor on the leading edge of efficiency, we strive to put into practice user-oriented capabilities and improvements regularly. We are always thankful for any feedback - play a pivotal part in revampimg the way you work with PDF documents. Should you be seeking to start, here's what it will take:
Step 1: Click the orange "Get Form" button above. It'll open up our editor so you could start filling in your form.
Step 2: Once you access the tool, there'll be the document ready to be filled out. Apart from filling out various blanks, you can also perform other sorts of things with the Document, specifically adding any text, editing the original textual content, inserting illustrations or photos, placing your signature to the PDF, and much more.
As for the blanks of this particular document, here is what you should do:
1. It is advisable to fill out the FRV accurately, hence pay close attention when working with the sections that contain all these blank fields:
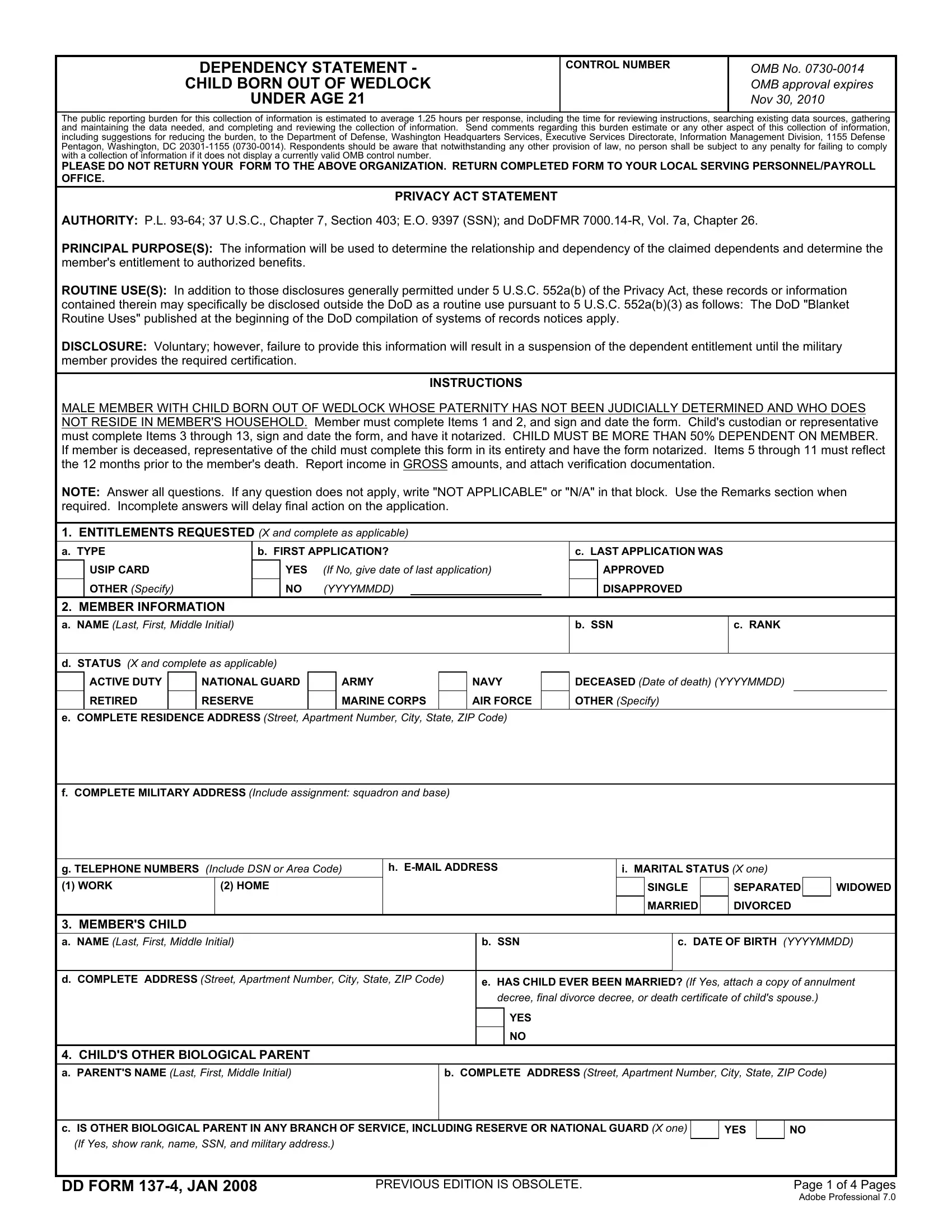
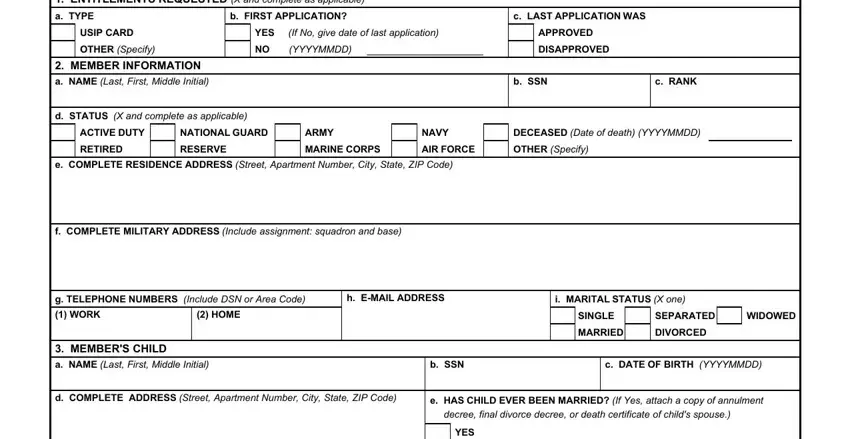
2. Your next step is usually to complete these fields: ENTITLEMENTS REQUESTED X and, a TYPE, b FIRST APPLICATION, c LAST APPLICATION WAS, USIP CARD, OTHER Specify, YES If No give date of last, NO YYYYMMDD, APPROVED, DISAPPROVED, MEMBER INFORMATION, a NAME Last First Middle Initial, d STATUS X and complete as, b SSN, and c RANK.
3. This next step is normally straightforward - complete all the fields in CHILDS OTHER BIOLOGICAL PARENT, a PARENTS NAME Last First Middle, b COMPLETE ADDRESS Street, c IS OTHER BIOLOGICAL PARENT IN, YES, If Yes show rank name SSN and, DD FORM JAN, PREVIOUS EDITION IS OBSOLETE, and Page of Pages Adobe Professional in order to complete this segment.
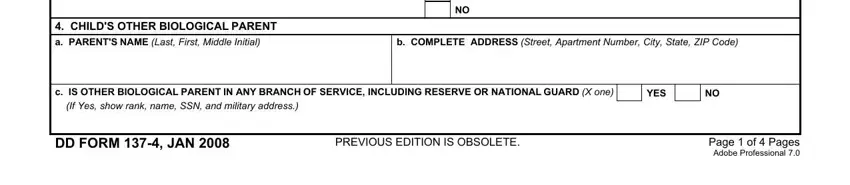
It is possible to make an error when completing the a PARENTS NAME Last First Middle, thus be sure to go through it again before you'll submit it.
4. The subsequent section requires your details in the following parts: CHILDS OTHER BIOLOGICAL PARENT, d DOES OTHER PARENT CLAIM CHILD, YES, If Yes explain, e WAS CHILDS MOTHER MARRIED FOR, YES, If the mother was married but is, f HAS PATERNITY OF CHILD BEEN, g HAS MEMBER BEEN JUDICIALLY, If Yes ID card can be issued, If Yes furnish a copy of all, YES, CHILDS RESIDENCE, a TYPE OF RESIDENCE X and complete, and YES. Be sure that you fill in all of the required details to go further.
5. To conclude your form, this last section has a few extra blank fields. Completing a NAME Last First Middle Initial, TO CHILD, c AGE, YES, HOURS PER WEEK, NO X, HOUSEHOLD EXPENSES, List the household expenses for, PRESENT MONTHLY, TOTAL EXPENSE FOR, EXPENSE, PAST MONTHS, ITEM, PRESENT MONTHLY, and TOTAL EXPENSE FOR will certainly wrap up everything and you can be done quickly!
Step 3: Just after going through the entries, click "Done" and you're good to go! Sign up with FormsPal today and instantly access FRV, available for downloading. All adjustments you make are saved , helping you to change the document later on if necessary. FormsPal is committed to the personal privacy of all our users; we make sure that all information put into our editor is secure.