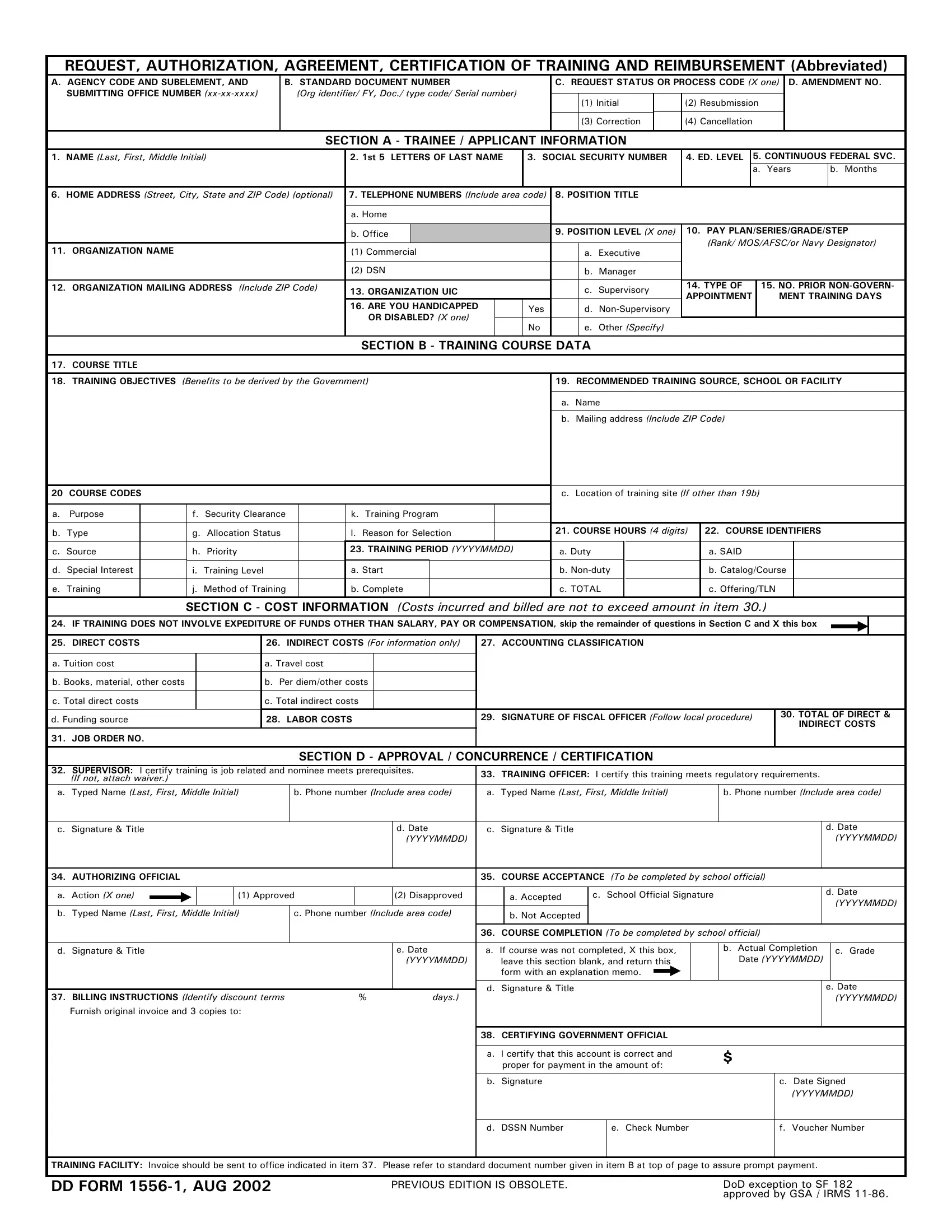
The DD Form 1556-1 serves as a comprehensive document designed for the request, authorization, agreement, certification of training, and reimbursement processes within the Department of Defense (DoD). This multifaceted form plays a crucial role in the facilitation of training requests for DoD personnel, encompassing everything from initial training requests to the final steps involving course completion evaluations and reimbursement details. It's meticulously structured to capture detailed trainee or applicant information, including but not limited to personal identification, federal service duration, and educational level. Furthermore, it addresses training course data, delving into course titles, objectives, and the recommended training facility, alongside a thorough breakdown of associated costs – direct, indirect, and labor. The form mandates official endorsements from supervisors, training officers, and authorizing officials to ensure the proposed training aligns with job requirements and regulatory standards. Additionally, it accommodates for the documentation of eventual course outcomes, completion status, and participant evaluations, thereby offering a holistic view of the training endeavor from inception to conclusion. Completing this form correctly is vital for DoD personnel seeking to pursue training opportunities, as it not only serves as a request but also contracts an agreement concerning the implications of such training on their service continuation and potential financial obligations.
| Question | Answer |
|---|---|
| Form Name | Dd Form 1556 1 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | OPM, dd form 1556, 1st, dd form 1556 1 |
REQUEST, AUTHORIZATION, AGREEMENT, CERTIFICATION OF TRAINING AND REIMBURSEMENT (Abbreviated)
A.AGENCY CODE AND SUBELEMENT, AND SUBMITTING OFFICE NUMBER
B. STANDARD DOCUMENT NUMBER
(Org identifier/ FY, Doc./ type code/ Serial number)
C. REQUEST STATUS OR PROCESS CODE (X one)
|
(1) |
Initial |
|
(2) |
Resubmission |
|
|
|
|
|
|
|
(3) |
Correction |
|
(4) |
Cancellation |
|
|
|
|
|
|
D. AMENDMENT NO.
SECTION A - TRAINEE / APPLICANT INFORMATION
1. NAME (Last, First, Middle Initial) |
2. 1st 5 LETTERS OF LAST NAME |
3. SOCIAL SECURITY NUMBER |
4. ED. LEVEL |
5. CONTINUOUS FEDERAL SVC. |
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
a. Years |
b. Months |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
6. HOME ADDRESS (Street, City, State and ZIP Code) (optional) |
7. TELEPHONE NUMBERS (Include area code) |
8. POSITION TITLE |
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
a. Home |
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
b. Office |
|
|
|
|
9. POSITION LEVEL (X one) |
10. |
PAY PLAN/SERIES/GRADE/STEP |
||||||
11. ORGANIZATION NAME |
|
|
(1) Commercial |
|
|
a. Executive |
|
(Rank/ MOS/AFSC/or Navy Designator) |
||||||||||
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
(2) DSN |
|
|
b. Manager |
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
12. ORGANIZATION MAILING ADDRESS (Include ZIP Code) |
13. ORGANIZATION UIC |
|
|
c. Supervisory |
14. TYPE OF |
|
15. NO. PRIOR |
|||||||||||
|
|
APPOINTMENT |
|
MENT TRAINING DAYS |
||||||||||||||
|
|
|
|
|
16. ARE YOU HANDICAPPED |
|
Yes |
|
d. |
|
|
|
|
|
|
|||
|
|
|
|
|
OR DISABLED? (X one) |
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
No |
|
e. Other (Specify) |
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SECTION B - TRAINING COURSE DATA |
|
|
|
|
|
|
|||||||
17. |
COURSE TITLE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
18. TRAINING OBJECTIVES (Benefits to be derived by the Government) |
|
19. RECOMMENDED TRAINING SOURCE, SCHOOL OR FACILITY |
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
a. Name |
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
b. Mailing address (Include ZIP Code) |
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
20 COURSE CODES |
|
|
|
|
|
|
|
c. Location of training site (If other than 19b) |
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
a. |
Purpose |
|
f. Security Clearance |
|
k. Training Program |
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
b. |
Type |
|
g. Allocation Status |
|
l. Reason for Selection |
|
|
21. COURSE HOURS (4 digits) |
22. COURSE IDENTIFIERS |
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
c. |
Source |
|
h. Priority |
|
23. TRAINING PERIOD (YYYYMMDD) |
|
a. Duty |
|
|
a. SAID |
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
d. |
Special Interest |
|
i. Training Level |
|
a. Start |
|
|
|
b. |
|
|
b. Catalog/Course |
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
e. |
Training |
|
j. Method of Training |
|
b. Complete |
|
|
|
c. TOTAL |
|
|
c. Offering/TLN |
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SECTION C - COST INFORMATION (Costs incurred and billed are not to exceed amount in item 30.)
24. IF TRAINING DOES NOT INVOLVE EXPEDITURE OF FUNDS OTHER THAN SALARY, PAY OR COMPENSATION, skip the remainder of questions in Section C and X this box
25. DIRECT COSTS |
|
|
26. INDIRECT COSTS (For information only) |
27. ACCOUNTING CLASSIFICATION |
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
a. Tuition cost |
|
|
a. Travel cost |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
b. Books, material, other costs |
|
|
b. Per diem/other costs |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
c. Total direct costs |
|
|
c. Total indirect costs |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
d. Funding source |
|
|
28. LABOR COSTS |
|
|
29. SIGNATURE OF FISCAL OFFICER (Follow local procedure) |
30. TOTAL OF DIRECT & |
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
INDIRECT COSTS |
|||
31. JOB ORDER NO. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SECTION D - APPROVAL / CONCURRENCE / CERTIFICATION |
|
|
|
|
|
|||||||||
32. SUPERVISOR: I certify training is job related and nominee meets prerequisites. |
33. TRAINING OFFICER: I certify this training meets regulatory requirements. |
|
|
|||||||||||||||||
(If not, attach waiver.) |
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
a. Typed Name (Last, First, Middle Initial) |
|
b. Phone number (Include area code) |
a. Typed Name (Last, First, Middle Initial) |
b. Phone number (Include area code) |
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
c. Signature & Title |
|
|
|
|
|
|
d. Date |
c. Signature & Title |
|
|
|
|
|
|
|
d. Date |
||||
|
|
|
|
|
|
|
|
|
(YYYYMMDD) |
|
|
|
|
|
|
|
|
|
|
(YYYYMMDD) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
34. AUTHORIZING OFFICIAL |
|
|
|
|
|
|
|
35. COURSE ACCEPTANCE (To be completed by school official) |
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
a. Action (X one) |
|
|
|
(1) Approved |
|
|
(2) Disapproved |
|
a. Accepted |
c. School Official Signature |
|
|
|
d. Date |
||||||
|
|
|
|
|
|
|
|
|
(YYYYMMDD) |
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
b. Typed Name (Last, First, Middle Initial) |
|
c. Phone number (Include area code) |
|
b. Not Accepted |
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
36. COURSE COMPLETION (To be completed by school official) |
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
d. Signature & Title |
|
|
|
|
|
|
e. Date |
a. If course was not completed, X this box, |
|
b. Actual Completion |
|
c. Grade |
||||||||
|
|
|
|
|
|
|
|
|
(YYYYMMDD) |
leave this section blank, and return this |
|
Date (YYYYMMDD) |
|
|
||||||
|
|
|
|
|
|
|
|
|
|
form with an explanation memo. |
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
d. Signature & Title |
|
|
|
|
|
|
|
e. Date |
||
37. BILLING INSTRUCTIONS (Identify discount terms |
% |
|
days.) |
|
|
|
|
|
|
|
|
|
|
(YYYYMMDD) |
||||||
Furnish original invoice and 3 copies to: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
38. CERTIFYING GOVERNMENT OFFICIAL |
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
a. I certify that this account is correct and |
$ |
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
proper for payment in the amount of: |
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
b. Signature |
|
|
|
|
|
c. Date Signed |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(YYYYMMDD) |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
d. DSSN Number
e. Check Number
f. Voucher Number
TRAINING FACILITY: Invoice should be sent to office indicated in item 37. Please refer to standard document number given in item B at top of page to assure prompt payment.
DD FORM |
PREVIOUS EDITION IS OBSOLETE. |
DoD exception to SF 182 |
|
|
approved by GSA / IRMS |
SECTION E - TERMINATION AND EVALUATION DATA (To be completed by trainee)
39. WAS COURSE COMPLETED (X one)
a. Yes |
(If not, return form with a |
|
|
b. No |
memo explaining circumstances) |
40. ACTUAL COURSE DATES (YYYYMMDD) |
41. ACTUAL COURSE HOURS |
||
|
|
|
|
a. Commenced |
b. Completed |
a. Duty |
b. |
|
|
|
|
42.ACADEMIC GRADE/ SCORE
43.WERE ALL SESSIONS ATTENDED? (X one)
a.Yes
b.No (Explain reason)
44.WHAT WERE YOUR OBJECTIVES IN TAKING THIS COURSE? WERE THEY MET?
|
|
AREAS OF EVALUATION |
|
|
|
RATING |
|
|
|
|
|
|
|
|
|
|
X appropriate column to indicate your evaluation of items 45 through 56. Do not attempt to split a rating. |
A |
B |
C |
|||
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
45. |
STATED OBJECTIVE ACCOMPLISHED |
A - Yes |
B - Partially |
C - No |
|
|
|
|
|
|
|
|
|
|
|
46. |
COVERAGE OF SUBJECT MATTER |
A - Excellent |
B - Sufficient |
C - Poor |
|
|
|
|
|
|
|
|
|
|
|
47. |
ORGANIZATION OF SUBJECT MATTER |
A - Well organized |
B - Adequate |
C - Poorly organized |
|
|
|
|
|
|
|
|
|
|
|
48. |
SUITABILITY OF INSTRUCTIONAL MATERIALS |
A - Excellent |
B - Adequate |
C - Poor |
|
|
|
|
|
|
|
|
|
|
|
49. |
LEVEL OF DIFFICULTY |
A - Too advanced |
B - Appropriate |
C - Too elementary |
|
|
|
|
|
|
|
|
|
|
|
50. |
LENGTH OF COURSE |
A - Too long |
B - Appropriate |
C - Too short |
|
|
|
|
|
|
|
|
|
|
|
51. |
AMOUNT OF OUTSIDE OR EVENING WORK |
A - Too much |
B - Appropriate |
C - Insufficient |
|
|
|
|
|
|
|
|
|
|
|
52. |
EFFECTIVENESS OF INSTRUCTORS |
A - Excellent |
B - Good |
C - Poor |
|
|
|
|
|
|
|
|
|
|
|
53. |
APPLICABILITY OF SUBJECT MATTER TO JOB |
A - Significant |
B - Adequate |
C - Insignificant |
|
|
|
|
|
|
|
|
|
|
|
54. |
FACILITIES |
A - Excellent |
B - Good |
C - Poor |
|
|
|
|
|
|
|
|
|
|
|
55. |
RECOMMENDATION TO COLLEAGUES |
A - Highly recommend |
B - Recommend |
C - Not recommended |
|
|
|
|
|
|
|
|
|
|
|
56. |
MEET CAREER DEVELOPMENT PLANS |
A - Yes |
B - No |
C - Not applicable |
|
|
|
|
|
|
|
|
|
|
|
57. COMMENTS ON COURSE STRENGTHS/WEAKNESSES
SECTION F - SUPERVISORY COMMENTS (To be completed by trainee's immediate supervisor)
58. HAVE YOU DISCUSSED THIS COURSE AND ITS APPLICATION TO THE JOB WITH THIS EMPLOYEE? (X one)
a. Yes
b. No
59.WHAT ARE YOUR OBJECTIVES IN HAVING EMPLOYEES ATTEND COURSE? (Complete at time of nomination)
60.WERE THE OBJECTIVES OF THE TRAINING ACHIEVED?
61.ADDITIONAL COMMENTS
62. SUPERVISOR
a. Signature
|
63. TRAINEE |
|
b. Date |
a. Signature |
|
(YYYYMMDD) |
|
|
|
|
b.Date (YYYYMMDD)
PRIVACY ACT STATEMENT
AUTHORITY: 5 U.S.C. Sections 4101 - 4118; and E.O. 9397.
PRINCIPAL PURPOSE(S): To request training by employees or military personnel and to document the authorization for expenses of such training; agreements for continuation in service following training, certificates of training, and any reimbursement obligations contracted by personnel or employees as a result of receiving training.
ROUTINE USE(S): Civilian training information is provided to Office of Personnel Management (OPM) for data reporting purposes stipulated in 5 U.S.C. 4115.
DISCLOSURE: Voluntary; however, failure to furnish the requested information may result in your ineligibility for participating in this training.
DD FORM