|
FOR OFFICIAL USE ONLY (When filled in) |
|
|
|
|
|
|
DETAILED INSTRUCTIONS (Continued) |
|
|
|
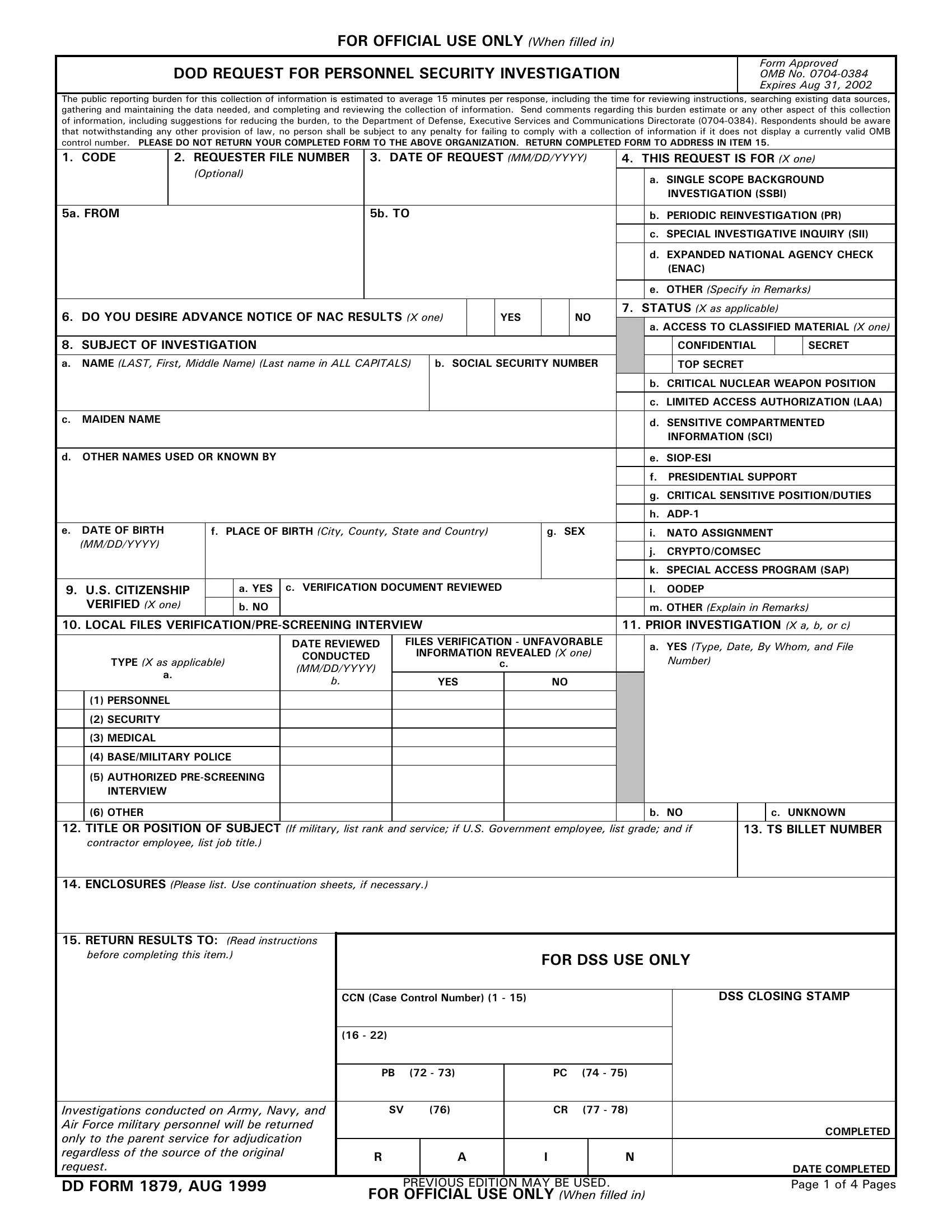
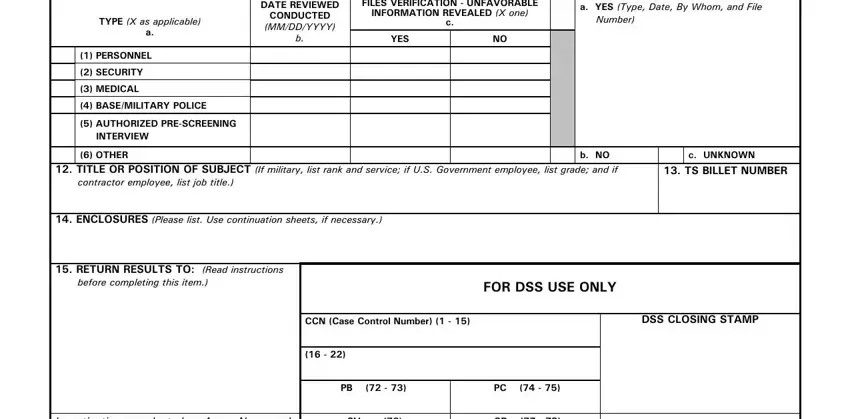
10. LOCAL FILES VERIFICATION/PRE-SCREENING INTERVIEW. |
16. REASON ACCESS TO CLASSIFIED INFORMATION OR |
Include a review of appropriate indices and files maintained by or for |
INVESTIGATION IS REQUIRED. |
|
the military or employing agency/activity concerning its person- nel. |
|
|
Examples are organization, management, and supervisor files; |
MILITARY/U.S. GOVERNMENT EMPLOYEES. List unclassified |
personnel, disciplinary, performance and counseling files; medical |
description of duties which warrant access to classified information |
files; special security and special program files; security, law en- |
or which warrant the investigation. |
|
forcement and intelligence indices or files (excluding state and local |
CONTRACTOR EMPLOYEES. List unclassified description of |
civilian law enforcement agencies); and legal and legal assistance |
duties which warrant access to classified information or which |
files (excluding statutorily restricted information). Included are files, |
warrant the investigation. Also, the applicable contract number |
forms or records executed by persons having knowledge of the |
MUST be listed. |
|
individual being considered for a personnel security investigation. |
|
|
Local files include files maintained by other elements of a corpora- |
17. HISTORY OF GOVERNMENT EMPLOYMENT AND/OR CURRENT |
tion or its parent company in support of the employing entity. |
MILITARY SERVICE INDICATED ON ATTACHED SF 85P/SF 86 IS: |
a. TYPE. |
|
MILITARY/U.S. GOVERNMENT EMPLOYEES. Complete as |
MILITARY/U.S. GOVERNMENT EMPLOYEES. The review of |
appropriate. If block 17.b. or 17.c. is marked, provide explanation |
local files will be indicated by marks in the appropriate blocks. If a |
in Item 18. |
|
particular record was not reviewed, indicate, in Item 18, the reason |
CONTRACTOR EMPLOYEES. This item MUST be left blank. |
why and state where the record is located. Complete block (5) if an |
|
|
Authorized Pre-Screening Interview was conducted; if not |
18. REMARKS. Enter information necessary to clarify entries in |
conducted when appropriate, indicate the reason in Item 18. |
other items and to list additional information when there is |
Complete block (6) if other records are reviewed that do not fall into |
insufficient space. This item may be continued on plain bond paper |
categories (1) through (5). |
|
with a heading containing subject's name, Social Security Number, |
CONTRACTOR EMPLOYEES. Mark blocks (1), (2), and (6), if |
and the notation "Continuation Sheet - 1879." |
|
appropriate. Also, mark block (3) if the information is available to |
|
|
you; if not, so indicate. Do not mark blocks (4) or (5). |
19. INVESTIGATION VALIDITY CERTIFICATION. |
|
b. DATE REVIEWED/CONDUCTED. Enter date review was |
|
|
completed for each record and, if applicable, date Pre-Screening |
a. TYPED NAME OF CERTIFIER. Type full name of individual |
Interview was conducted. |
|
certifying validity of the request for investigation. |
|
c. FILES VERIFICATION - UNFAVORABLE INFORMATION |
CONTRACTOR EMPLOYEES. If the request is for a Top Secret |
REVEALED. |
|
MILITARY/U.S. GOVERNMENT EMPLOYEES. Mark as applicable |
clearance, this individual must be the Facility Security Officer (FSO) |
for each type of record and/or Pre-Screening Interview. If |
or other OODEP. For all other requests, this individual must be the |
unfavorable information is developed, provide pertinent details in |
FSO or a designee. |
|
Item 18. |
|
|
|
CONTRACTOR EMPLOYEES. Mark as applicable for each type |
b. TITLE OF CERTIFIER. List the title of individual certifying the |
of record. If unfavorable information is developed, provide pertinent |
request for investigation. |
|
details in Item 18. |
|
c. SIGNATURE OF CERTIFIER. Signature of individual authorized |
|
|
11. PRIOR INVESTIGATION. |
|
to request investigation. |
|
MILITARY/U.S. GOVERNMENT EMPLOYEES, AND |
|
|
CONTRACTOR EMPLOYEES. If "Yes," be sure that the type of |
d. DATE SIGNED BY CERTIFIER. Enter the date this form is |
investigation, date, who conducted the investigation, and the file |
signed. |
|
number are listed. |
|
e. TELEPHONE NUMBER. List the telephone number, including |
|
|
12. TITLE OR POSITION OF SUBJECT. |
|
area code and/or Defense Switched Network (DSN) of the certifying |
MILITARY OR U.S. GOVERNMENT EMPLOYEES. If military |
official. |
|
service member, list rank, service and write in "Military Applicant." |
|
|
If U.S. Government Employee, list grade and write in "U.S. |
20. EMPLOYEE'S IMMEDIATE SUPERVISOR'S CERTIFICATION. |
Government Applicant." |
|
If request is for an upgrading of a currently held clearance or for a |
CONTRACTOR EMPLOYEES. List job title. |
Periodic Reinvestigation (PR), the subject's immediate supervisor |
|
|
MUST complete the certification. Certification by the immediate |
13. TS BILLET NUMBER. |
|
supervisor does not require review of the completed SF 85P/SF 86 |
MILITARY/U.S. GOVERNMENT EMPLOYEES. If request is for a |
by the supervisor. |
|
Top Secret clearance, list the Billet Number if such a system has |
If the electronic DD Form 1879 is utilized, the requester must |
been implemented. |
|
retain an originally signed document from the employee's immediate |
CONTRACTOR EMPLOYEES. This item should be left blank. |
supervisor certifying the absence or presence of any adverse |
14. ENCLOSURES. List and identify all enclosures attached to this |
information. This documentation must be retained with a copy of |
the electronically generated DD Form 1879, signed by the |
form (i.e., SF 85P, SF 86, FD Form 258, copies of local files |
requester, until the clearance process is complete. The employee's |
verification, results of Pre-Screening Interview, etc.). |
immediate supervisor documentation must contain the following: |
15. RETURN RESULTS TO. |
|
a. ADVERSE INFORMATION. Self-explanatory. |
|
MILITARY PERSONNEL. Enter the name of the parent military |
|
|
service which will adjudicate the investigation. NOTE: Investiga- |
b. IMMEDIATE SUPERVISOR. Type full name of immediate |
tions conducted on military personnel, who are assigned to a DoD |
supervisor. |
|
Component, will be returned only to the Subject's parent military |
|
|
service for adjudication, regardless of the Component making the |
c. TITLE. List the title of immediate supervisor. |
|
original request. The adjudicating facility will then be responsible |
|
|
for expeditiously transmitting the results of the clearance deter- |
d. SIGNATURE. Signature of immediate supervisor. |
mination to the Component who requested the investigation. |
|
|
U.S. GOVERNMENT EMPLOYEES. Enter the name of the |
e. DATE SIGNED. Enter the date this form is signed. |
organization and mailing address that the investigation should be |
|
|
sent to upon completion. |
|
f. TELEPHONE NUMBER. List the telephone number, including |
CONTRACTOR EMPLOYEES. This item MUST be left blank. |
area code and/or DSN number of the immediate supervisor. |
|
|
|
|
DD FORM 1879, AUG 1999 |
FOR OFFICIAL USE ONLY (When filled in) |
Page 4 of 4 Pages |