



If you need to fill out 2004, you don't have to install any kind of software - simply give a try to our online PDF editor. To have our tool on the cutting edge of convenience, we aim to implement user-oriented capabilities and enhancements regularly. We are routinely looking for feedback - join us in reshaping how you work with PDF documents. Here is what you will want to do to begin:
Step 1: Click the orange "Get Form" button above. It will open our tool so you could begin filling in your form.
Step 2: The editor provides you with the capability to customize PDF forms in a variety of ways. Transform it by including your own text, correct existing content, and place in a signature - all at your convenience!
It will be simple to complete the document using this helpful guide! Here's what you need to do:
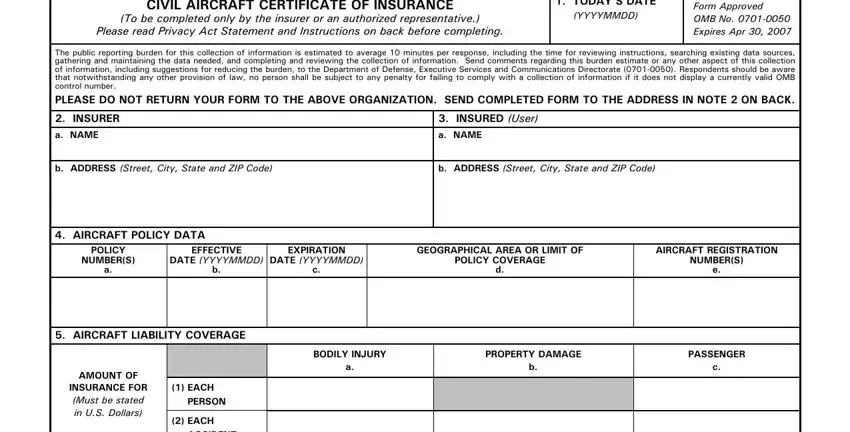
1. Before anything else, once filling in the 2004, beging with the part that features the next fields:
2. Given that the last array of fields is complete, it is time to include the necessary particulars in SINGLE LIMIT If the aircraft are, bodily injury property damage and, EXCESS LIABILITY If the aircraft, PROVISIONS OF AMENDMENTS OR, a The insurer waives any right of, b The insurance afforded by the, c If the insurer cancels or, d If the insured requests, CERTIFICATION To be completed by, I certify that insurance is in, a TYPED NAME OF INSURERS, and b SIGNATURE Blue Ink so you can go further.
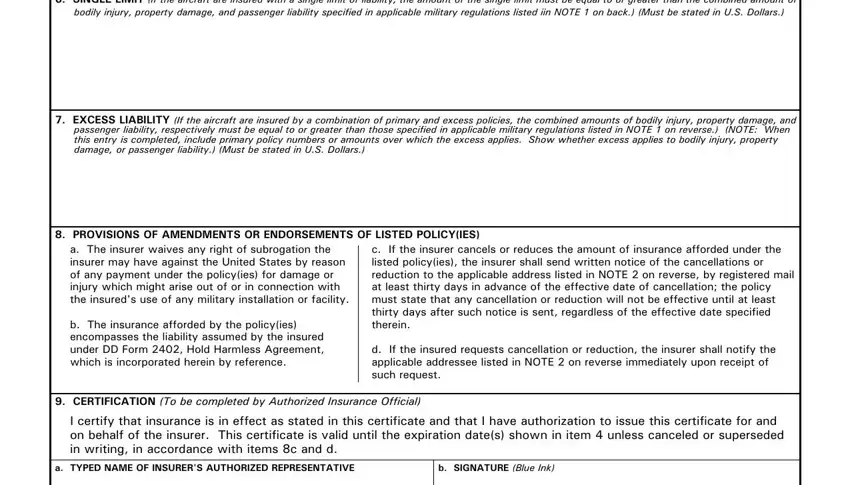
It's simple to make a mistake when filling in your CERTIFICATION To be completed by, for that reason you'll want to reread it before you decide to submit it.
3. Completing c TITLE, d TELEPHONE NUMBER Include Area, DD FORM AUG, and PREVIOUS EDITION IS OBSOLETE is essential for the next step, make sure to fill them out in their entirety. Don't miss any details!

4. Completing IF ADDITIONAL SPACE IS REQUIRED, ARMY, NAVY, AIR FORCE, NOTE, AR Can be viewed at, SECNAVINST C Can be viewed at, and AFI Can be viewed at is essential in the next stage - be sure to devote some time and be attentive with every single blank!
Step 3: Be certain that your details are accurate and then click "Done" to finish the task. Create a 7-day free trial subscription with us and get immediate access to 2004 - download, email, or edit in your personal account. Whenever you work with FormsPal, you can certainly complete documents without stressing about information leaks or records being distributed. Our secure platform ensures that your private information is stored safe.