
Any time you need to fill out dd 2790, you won't have to download any kind of software - just try our online tool. In order to make our tool better and less complicated to utilize, we consistently come up with new features, with our users' suggestions in mind. Here's what you would want to do to get going:
Step 1: Click the orange "Get Form" button above. It'll open up our pdf editor so that you can start completing your form.
Step 2: With our advanced PDF file editor, you may accomplish more than just complete blanks. Express yourself and make your forms look sublime with custom textual content incorporated, or modify the original content to excellence - all comes with an ability to insert stunning photos and sign the PDF off.
With regards to the blanks of this particular form, here's what you should know:
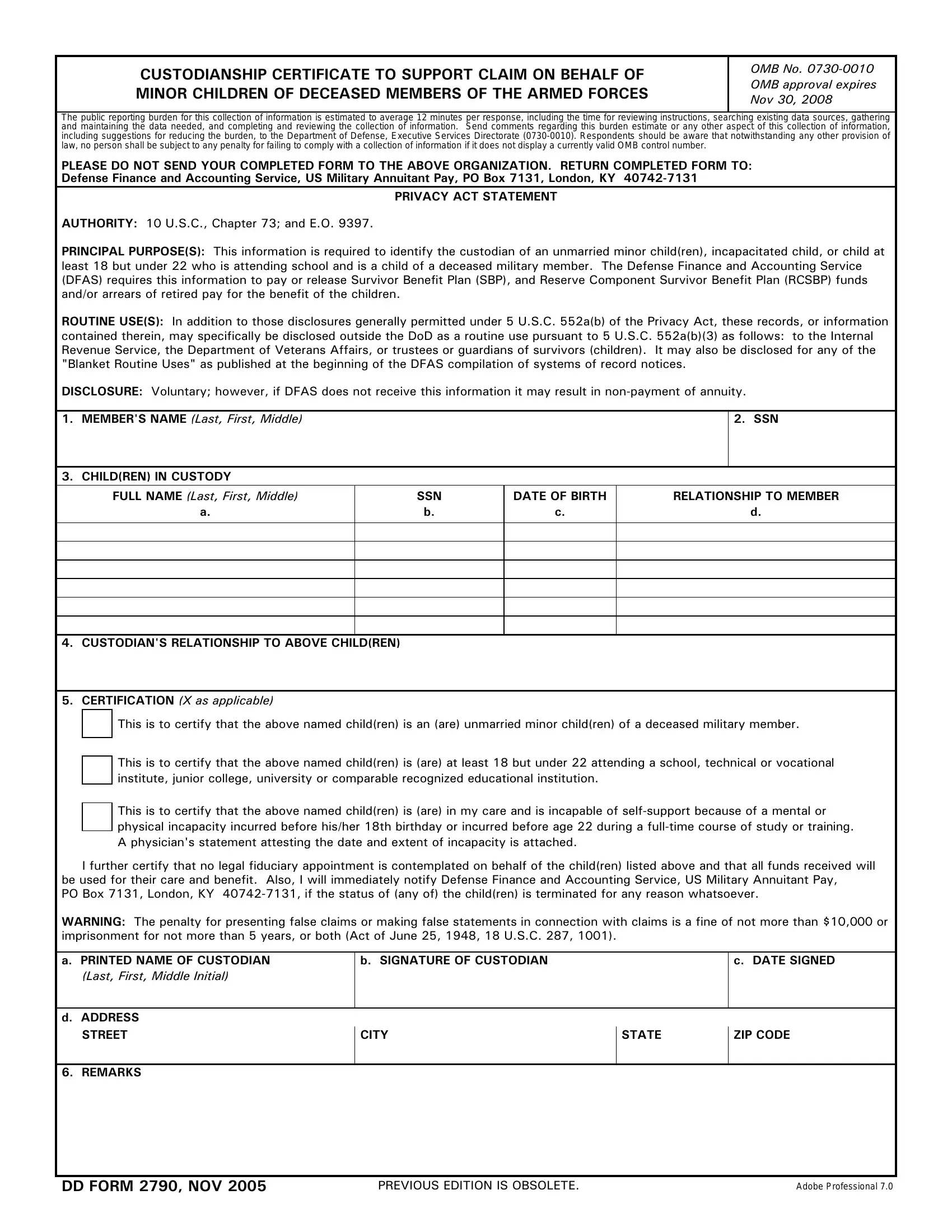
1. You will need to complete the dd 2790 correctly, so take care while filling in the parts that contain these specific blanks:
2. Soon after finishing this section, head on to the next step and enter the essential details in these blanks - a PRINTED NAME OF CUSTODIAN, Last First Middle Initial, b SIGNATURE OF CUSTODIAN, c DATE SIGNED, d ADDRESS, STREET, REMARKS, CITY, STATE, ZIP CODE, DD FORM NOV, PREVIOUS EDITION IS OBSOLETE, and Adobe Professional.
Be extremely attentive when completing b SIGNATURE OF CUSTODIAN and STREET, as this is the part where a lot of people make some mistakes.
Step 3: Soon after double-checking the entries, click "Done" and you are done and dusted! Go for a 7-day free trial account at FormsPal and gain instant access to dd 2790 - downloadable, emailable, and editable inside your personal account. FormsPal guarantees protected form completion without personal data recording or any sort of sharing. Rest assured that your details are secure with us!