CUI (when filled in)
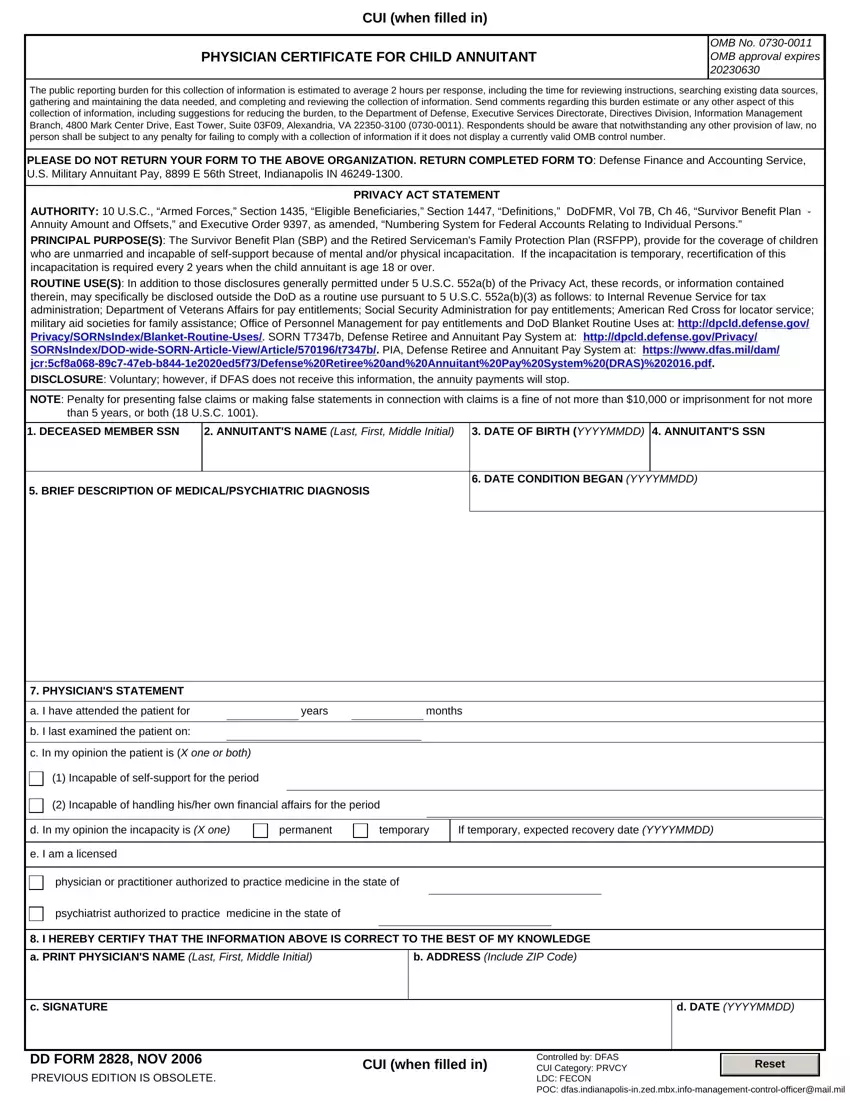
PHYSICIAN CERTIFICATE FOR CHILD ANNUITANT |
OMB No. 0730-0011 |
OMB approval expires |
|
20230630 |
The public reporting burden for this collection of information is estimated to average 2 hours per response, including the time for reviewing instructions, searching existing data sources, gathering and maintaining the data needed, and completing and reviewing the collection of information. Send comments regarding this burden estimate or any other aspect of this collection of information, including suggestions for reducing the burden, to the Department of Defense, Executive Services Directorate, Directives Division, Information Management Branch, 4800 Mark Center Drive, East Tower, Suite 03F09, Alexandria, VA 22350-3100 (0730-0011). Respondents should be aware that notwithstanding any other provision of law, no person shall be subject to any penalty for failing to comply with a collection of information if it does not display a currently valid OMB control number.
PLEASE DO NOT RETURN YOUR FORM TO THE ABOVE ORGANIZATION. RETURN COMPLETED FORM TO: Defense Finance and Accounting Service, U.S. Military Annuitant Pay, 8899 E 56th Street, Indianapolis IN 46249-1300.
PRIVACY ACT STATEMENT
AUTHORITY: 10 U.S.C., “Armed Forces,” Section 1435, “Eligible Beneficiaries,” Section 1447, “Definitions,” DoDFMR, Vol 7B, Ch 46, “Survivor Benefit Plan - Annuity Amount and Offsets,” and Executive Order 9397, as amended, “Numbering System for Federal Accounts Relating to Individual Persons.”
PRINCIPAL PURPOSE(S): The Survivor Benefit Plan (SBP) and the Retired Serviceman's Family Protection Plan (RSFPP), provide for the coverage of children who are unmarried and incapable of self-support because of mental and/or physical incapacitation. If the incapacitation is temporary, recertification of this incapacitation is required every 2 years when the child annuitant is age 18 or over.
ROUTINE USE(S): In addition to those disclosures generally permitted under 5 U.S.C. 552a(b) of the Privacy Act, these records, or information contained
therein, may specifically be disclosed outside the DoD as a routine use pursuant to 5 U.S.C. 552a(b)(3) as follows: to Internal Revenue Service for tax administration; Department of Veterans Affairs for pay entitlements; Social Security Administration for pay entitlements; American Red Cross for locator service; military aid societies for family assistance; Office of Personnel Management for pay entitlements and DoD Blanket Routine Uses at: http://dpcld.defense.gov/ Privacy/SORNsIndex/Blanket-Routine-Uses/. SORN T7347b, Defense Retiree and Annuitant Pay System at: http://dpcld.defense.gov/Privacy/ SORNsIndex/DOD-wide-SORN-Article-View/Article/570196/t7347b/. PIA, Defense Retiree and Annuitant Pay System at: https://www.dfas.mil/dam/ jcr:5cf8a068-89c7-47eb-b844-1e2020ed5f73/Defense%20Retiree%20and%20Annuitant%20Pay%20System%20(DRAS)%202016.pdf.
DISCLOSURE: Voluntary; however, if DFAS does not receive this information, the annuity payments will stop.
NOTE: Penalty for presenting false claims or making false statements in connection with claims is a fine of not more than $10,000 or imprisonment for not more than 5 years, or both (18 U.S.C. 1001).
1. DECEASED MEMBER SSN |
2. ANNUITANT'S NAME (Last, First, Middle Initial) 3. DATE OF BIRTH (YYYYMMDD) 4. ANNUITANT'S SSN |
6. DATE CONDITION BEGAN (YYYYMMDD)
5. BRIEF DESCRIPTION OF MEDICAL/PSYCHIATRIC DIAGNOSIS
|
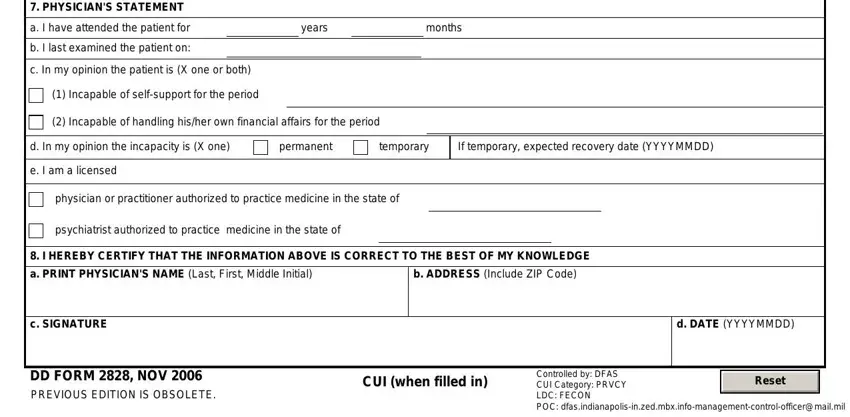
7. PHYSICIAN'S STATEMENT |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
a. I have attended the patient for |
|
|
years |
|
|
|
|
months |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
b. I last examined the patient on: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
c. In my opinion the patient is (X one or both) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(1) Incapable of self-support for the period |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(2) Incapable of handling his/her own financial affairs for the period |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
d. In my opinion the incapacity is (X one) |
permanent |
|
temporary |
If temporary, expected recovery date (YYYYMMDD) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
e. I am a licensed |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
physician or practitioner authorized to practice medicine in the state of |
|
|
|
|
|
|
|
|
|
|
psychiatrist authorized to practice medicine in the state of |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
8. I HEREBY CERTIFY THAT THE INFORMATION ABOVE IS CORRECT TO THE BEST OF MY KNOWLEDGE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
a. PRINT PHYSICIAN'S NAME (Last, First, Middle Initial) |
|
|
b. ADDRESS (Include ZIP Code) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
c. SIGNATURE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
d. DATE (YYYYMMDD) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DD FORM 2828, NOV 2006 |
|
|
|
CUI (when filled in) |
Controlled by: DFAS |
|
|
|
|
|
|
|
|
|
|
Reset |
|
|
|
|
|
|
|
CUI Category: PRVCY |
|
|
|
PREVIOUS EDITION IS OBSOLETE. |
|
|
|
|
|
|
|
|
|
|
|
LDC: FECON |
|
|
|
|
|
POC: dfas.indianapolis-in.zed.mbx.info-management-control-officer@mail.mil