The Department of Defense Form 2911, also known as the Certificate of Release or Discharge from Active Duty, is a document that is issued to active duty military personnel upon their separation from the service. The form includes details such as the servicemember's name, rank, military occupation specialty code (MOS), and dates of active duty service. It can be used to establish veterans' benefits and may be required for other purposes such as re-enlistment or public employment. The Form 2911 must be signed by the servicemember and dated within 90 days of discharge.
| Question | Answer |
|---|---|
| Form Name | Dd Form 2911 |
| Form Length | 15 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 3 min 45 sec |
| Other names | YYYYMMDD, DF, SHX, anoscopic |
DoD SEXUAL ASSAULT FORENSIC EXAMINATION REPORT
PRIVACY ACT STATEMENT |
|
AUTHORITY: Section 301 of Title 5 U.S.C. and Chapter 55 of Title 10 U.S.C.; DoDD 6495.01, Sexual |
|
Assault Prevention and Response (SAPR) Program; and DoDI 6495.02 Sexual Assault Prevention and |
|
Response Program Procedures. |
|
PRINCIPAL PURPOSE(S): Information on this form will be used to document the medical/forensic |
|
examination of the sexual assault victim. The DD Form 2911 also documents the reporting preference |
|
(Restricted or Unrestricted) of the sexual assault victim as part of the sexual assault prevention and |
|
response program. |
|
ROUTINE USE(S): None. |
|
DISCLOSURE: Completion of this form is voluntary; however, failure to complete this form with the |
|
information requested impedes the effective management of care and support required by the |
|
procedures of the sexual assault prevention and response program. |
Patient Identification |
|
Sensitive Information Document
PART I (NOTE: Conduct a SAFE for up to one full week following a sexual assault, or longer if circumstances dictate.)
A. GENERAL INFORMATION (Print or type)
Name of Medical Facility:
1a. |
NAME OF PATIENT (Last, First, Middle Initial) |
|
|
|
|
|
b. PATIENT ID NUMBER |
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2a. |
ADDRESS |
|
b. CITY |
|
c. COUNTY |
|
d. STATE |
e. ZIP CODE |
f. TELEPHONE (Include Area Code) |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
(1) Home: |
||
|
|
|
|
|
|
|
|
|
|
|
|
(2) |
Work: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3a. |
AGE |
b. DATE OF BIRTH |
c. GENDER (X) |
d. ETHNICITY (X) |
e. RACE (X) |
|
|
|
|
|||||
|
|
(YYYY/MM/DD) |
M |
(1) Hispanic or |
|
|
(1) American Indian/ |
(3) Black or African |
(5) Native Hawaiian/ |
|||||
|
|
|
|
|||||||||||
|
|
|
Latino |
|
|
Alaska Native |
American |
|
|
Other Pacific Islander |
||||
|
|
|
|
|
|
|
|
|
||||||
|
|
|
F |
(2) Not Hispanic or |
|
|
(2) Asian |
(4) White |
|
|
|
|||
|
|
|
Latino |
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
||
4a. ARRIVAL DATE (YYYY/MM/DD) |
b. TIME |
|
|
5a. DISCHARGE DATE (YYYY/MM/DD) |
|
|
b. TIME |
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
B. NOTIFICATION AND AUTHORIZATION:
Location of Assault: |
|
Jurisdiction: |
|
|||||||
|
|
On Installation |
|
Off Installation |
|
|
City |
|
|
County |
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
Civilian or Foreign Assisting Agency:
Other
1a. NAME OF SEXUAL ASSAULT RESPONSE COORDINATOR (SARC) (Last, First, Middle Initial)
b.TELEPHONE (Include Area Code)
2a. NAME OF SEXUAL ASSAULT FORENSIC EXAMINER
(Last, First, Middle Initial)
b. RANK
c. TITLE
d.TELEPHONE (Include Area Code)
3a. NAME OF VICTIM ADVOCATE (VA) (Last, First, Middle Initial) |
|
b. TELEPHONE (Include Area Code) |
|
||||||
|
|
|
|
|
|
|
|
|
|
4a. NAME OF MILITARY CRIMINAL INVESTIGATIVE OFFICER (UNRESTRICTED REPORT) |
b. TELEPHONE (Include Area Code) |
|
|||||||
(Last, First, Middle Initial) |
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
c. AGENCY |
|
|
|
d. ID NUMBER |
|
e. DATE (YYYY/MM/DD) |
|
||
|
|
|
|
||||||
5a. NAME OF SERVICE DESIGNATED EVIDENCE COLLECTING OFFICER (RESTRICTED REPORT) |
|
b. TELEPHONE (Include Area Code) |
|||||||
(Last, First, Middle Initial) |
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
c. AGENCY |
|
|
d. ID NUMBER |
e. DATE (YYYY/MM/DD) |
f. TIME |
g. RESTRICTED REPORT |
|||
|
|
|
|
|
|
|
|
CONTROL NUMBER (RRCN) |
|
|
|
|
|
|
|
|
|
|
|
C. REPORTING INFORMATION |
|
|
|
|
|
|
|
||
|
|
|
|
|
|
||||
1. In unrestricted reporting, I understand that Military Medical Treatment Facilities and Healthcare Providers are required by Department of |
(Initial) |
||||||||
Defense regulations to report sexual assaults to Military Criminal Investigative Organization authorities (e.g., CID, NCIS, AFOSI). Under |
|
||||||||
these circumstances, the report must state the name of the injured person, current whereabouts, and the type and extent of injuries. |
|
||||||||
In Restricted reporting, I understand that Military Medical Treatment Facilities and Healthcare Providers are required by Department of |
|
||||||||
Defense regulations to report sexual assaults to the Sexual Assault Response Coordinator (SARC). |
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
2. The Sexual Assault Response Coordinator (SARC) and/or Victim Advocate (VA) have explained the difference between Unrestricted and |
(Initial) |
||||||||
|
|||||||||
Restricted Reporting options. I have elected: |
|
|
|
|
|||||
|
|
UNRESTRICTED REPORTING |
|
RESTRICTED REPORTING (Only applicable to Active Duty, and Reserve and National |
|
||||
|
|
|
|
||||||
Guard in active service or inactive duty training)
Note: Military dependents under age 18 who have been sexually assaulted by either parent and/or caregiver are not covered under the sexual assault restricted reporting policy.
(Initial)
3.I understand what my options are and do not have questions.
DD FORM 2911, SEP 2011 |
Page 1 of 14 Pages |
Adobe Professional 8.0
D. PATIENT CONSENT |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
1. I understand that the Sexual Assault Forensic Examination |
|
|
YES |
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
(also known as a "SAFE") that I am about to undergo is |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
optional. When I give my consent, a healthcare |
|
|
NO |
|
|
|
|
|
professional may examine me to find and collect evidence |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
of an assault. I understand that as part of the examination, |
|
(Initial) |
|
|
|
|
|
|
the provider can collect specimens to include my hair, urine |
|
|
|
|
|
|
|
|
and/or blood, both now and at a later date, if necessary. |
|
|
|
|
|
|
|
|
|
|
|
|
Patient Identification |
||||
|
|
|
|
|
|
|
|
(Initial) |
2. I understand that I may withdraw my consent at any time for any portion of the examination and that it |
|
YES |
||||||
|
|
|
|
|||||
|
|
|
|
|||||
will not impact my right to medical care. |
|
|
|
|
|
NO |
||
|
|
|
|
|
||||
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(Initial) |
3. I understand that collection of evidence may include photographing injuries and that these photographs |
|
YES |
||||||
|
|
|
|
|||||
|
|
|
|
|||||
may include the genital area. |
|
|
|
|
|
NO |
||
|
|
|
|
|
||||
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(Initial) |
4. I understand that samples of my blood and/or urine may need to be tested for drugs as part of my |
|
YES |
||||||
treatment. I also understand that testing for drugs will also show prescriptions, other drugs, and |
|
|||||||
|
|
|
|
|||||
|
|
|
|
|
|
|||
alcohol that I have voluntarily consumed. I understand that illegal drugs or alcohol (if I am under |
|
|
|
|
||||
age 21) in my body could be used to show that I engaged in misconduct if I am a Service member. |
|
NO |
||||||
I consent to this testing and the release of the result to law enforcement. |
|
|
|
|
||||
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(Initial) |
|
|
|
|
|
|
|||
5. I understand that some of the information that I provide may be collected for health and forensic |
|
YES |
||||||
purposes and provided to health authorities and other qualified persons for a valid educational or |
|
|||||||
|
|
|
|
|||||
|
|
|
|
|||||
|
|
|
|
|
|
|||
scientific interest and/or epidemiological studies. However, none of my personally identifying data |
|
NO |
||||||
(name, patient identification number, etc.) will be disclosed for these purposes. |
|
|||||||
|
|
|
|
|||||
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(Initial) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
YES |
||
6.I hereby consent to a sexual assault medical forensic examination (SAFE).
NO
|
|
(Initial) |
7. If I have elected to make an Unrestricted Report, I understand and consent to the release of my records |
|
YES |
|
|
|
|
|
|
and all evidence collected from this exam to law enforcement. |
|
NO |
|
||
|
|
|
|
|
|
8. If I have elected to make a Restricted Report, I understand that my records and all evidence collected |
|
YES |
(Initial) |
|||
|
|
|||||
|
|
|
||||
|
|
|
||||
|
should not be reviewed or tested unless I choose to convert to an Unrestricted Report. |
|
|
NO |
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
9a. |
PATIENT SIGNATURE |
|
b. DATE |
c. TIME |
||
|
|
|
(YYYY/MM/DD) |
|
||
|
|
|
|
|
|
|
10. |
PATIENT PARENT OR GUARDIAN (If applicable) |
|
|
|
|
|
a. SIGNATURE |
b. ADDRESS (If different from patient) (Include ZIP Code) |
c. DATE |
d. TIME |
|||
|
|
|
(YYYY/MM/DD) |
|
||
|
|
|
|
|
|
|
11. |
WITNESS TO PATIENT SIGNATURE |
|
|
|
|
|
a. SIGNATURE |
b. ADDRESS (Include ZIP Code) |
c. DATE |
d. TIME |
|||
|
|
|
(YYYY/MM/DD) |
|
||
|
|
|
|
|
|
|
DD FORM 2911, SEP 2011 |
Page 2 of 14 Pages |
E. PATIENT HISTORY |
|
|
|
|
|
|
|
|
|
|
|
|
|
1a. NAME OF PERSON PROVIDING HISTORY (Last, First, Middle Initial) |
|
|||||
|
|
|
|
|
|
|
b. RELATIONSHIP TO PATIENT |
|
|
|
c. DATE (YYYY/MM/DD) |
d. TIME |
|
|
|
|
|
|
|
|
2. PERTINENT MEDICAL HISTORY |
|
Patient Identification |
||||
a. LAST MENSTRUAL PERIOD |
b. Any recent (60 days) |
|||||
|
|
current physical findings? (If yes, describe) |
||||
|
|
|
No |
|
|
|
|
|
|
|
|
||
|
|
|
Yes |
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
c. Any other pertinent medical condition(s) that may affect the interpretation of current physical findings? (If yes, describe)
No
Yes
d. Any
No
Yes
3. PERTINENT
a. Other
|
|
No |
|
Yes |
|
Unsure |
If yes or unsure, complete items b. through f. below. If no, then check the "No" box to the left and proceed to item 4. |
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
(X and complete as applicable) |
No |
|
Yes |
Unsure |
(If Yes) |
|
|
|
|
|
|||||||||||
b. Anal (within past 5 days)? |
|
|
|
|
|
|
|
When? |
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
c. Vaginal (within past 5 days)? |
|
|
|
|
|
|
|
When? |
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
d. Oral (within past 5 days)? |
|
|
|
|
|
|
|
When? |
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
e. Did ejaculation occur? |
|
|
|
|
|
|
|
Where? |
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
f. Was a condom used? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4. |
|
|
Not Applicable if over 5 days |
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(X and complete as applicable) |
|
|
|
|
|
|
|
|
No |
Yes |
|
|
No |
Yes |
|||||||
a. Urinated |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
h. |
Brushed teeth |
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
b. Defecated |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
i. |
Gargled/mouthwash |
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
c. Genital or body wipes (If yes, describe) |
|
|
|
|
|
|
|
j. |
Vomited |
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
k. Ate or drank |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
d. Douched (If yes, with what) |
|
|
|
|
|
|
|
|
|
|
l. Used cream/ointment/lotion on body part involved in assault (If yes, |
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
describe) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
e. Removed/inserted |
|
|
|
|
|
|
|
|
|
|
m. Changed clothing (If yes, describe) |
|
|
||||||||
|
|
Tampon |
|
|
Diaphragm |
|
|
Nuva ring |
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
f. |
Oral gargle/rinse |
|
|
|
|
|
|
|
|
|
|
n. Changed body piercings (If yes, describe) |
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
g. |
Bath/shower/wash |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
F. ASSAULT HISTORY
1a. DATE OF ASSAULT(S) (YYYY/MM/DD) 2. LOCATION AND PERTINENT PHYSICAL SURROUNDINGS
b. TIME
3. PHYSICAL EFFECTS OF ASSAULT. If injuries are described or if remarkable findings or possible trauma are observed, please photograph.
a.
No
Yes
b. Genital/rectal injury, pain and/or bleeding (including tenderness). (If yes, describe.)
No
Yes
4. INJURIES INFLICTED UPON THE ASSAILANT(S) DURING ASSAULT? (If yes, describe injuries, possible locations on the body, and how they were inflicted.)
No
Yes
5a. NUMBER OF ASSAILANT(S) |
b. ASSAILANT(S) RELATIONSHIP TO VICTIM (Indicate/number all that apply) |
||||||||||
|
|
|
Stranger |
|
|
Acquaintance |
|
Relative (Specify) |
|||
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Other (Specify) |
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
DD FORM 2911, SEP 2011 |
Page 3 of 14 Pages |
G. PATIENT'S DESCRIPTION OF THE ASSAULT
Please record the patient's description of the assault.
Add additional pages if necessary.
Patient Identification
DD FORM 2911, SEP 2011 |
Page 4 of 14 Pages |
H. ACTS DESCRIBED BY PATIENT
- Describe any penetration of the genital, anal or oral opening, no matter how slight or brief.
- Type of sexual intercourse (oral, vaginal, anal).
- If more than one assailant, identify by number.
Patient Identification
|
1. PENETRATION OF VAGINA BY |
No |
Yes |
Attempted |
Unsure |
Describe: |
|||||||
|
a. Penis |
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|||||
|
b. Finger |
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|||||
|
c. Object (If yes, describe the object) |
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2. PENETRATION OF ANUS BY |
No |
Yes |
Attempted |
Unsure |
Describe: |
|||||||
|
a. Penis |
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|||||
|
b. Finger |
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|||||
|
c. Object (If yes, describe the object) |
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3. ORAL COPULATION OF GENITALS |
No |
Yes |
Attempted |
Unsure |
Describe: |
|||||||
|
a. Of patient by assailant |
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|||||||
|
b. Of assailant by patient |
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4. ORAL COPULATION OF ANUS |
No |
Yes |
Attempted |
Unsure |
Describe: |
|||||||
|
a. Of patient by assailant |
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|||||||
|
b. Of assailant by patient |
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
5. |
No |
Yes |
Attempted |
Unsure |
Describe: |
|||||||
|
a. Licking |
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|||||
|
b. Kissing |
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|||||
|
c. Suction injury |
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|||||
|
d. Biting |
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|||||
|
e. Strangulation/choking |
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
6. OTHER ACT(S) (Describe) |
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
7. DID EJACULATION OCCUR? |
No |
Yes |
Unsure |
|
|
|
||||||
|
|
(If yes, location(s)) |
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
Mouth |
|
|
Rectum |
|
|
|
|
|
|
|
|
|
|
|
|
|
Other (note location(s)) |
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Vagina |
|
|
Body surface |
|
|
|
|
|
|
|
|
|
|
Genitals |
|
|
On clothing |
|
|
|
|
|
|
|
|
|
|
Anus |
|
|
On bedding |
|
|
|
|
|
|
|
|
8. CONTRACEPTIVE OR LUBRICANT PRODUCT(S) |
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
No |
Yes |
Unsure |
Describe Type/Brand, if known: |
||
|
a. Condom used? |
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|||||
|
b. Lubricant used? |
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|||||
|
c. Other Contraceptive used? |
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DD FORM 2911, SEP 2011 |
Page 5 of 14 Pages |
|
I. GENERAL PHYSICAL EXAMINATION |
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
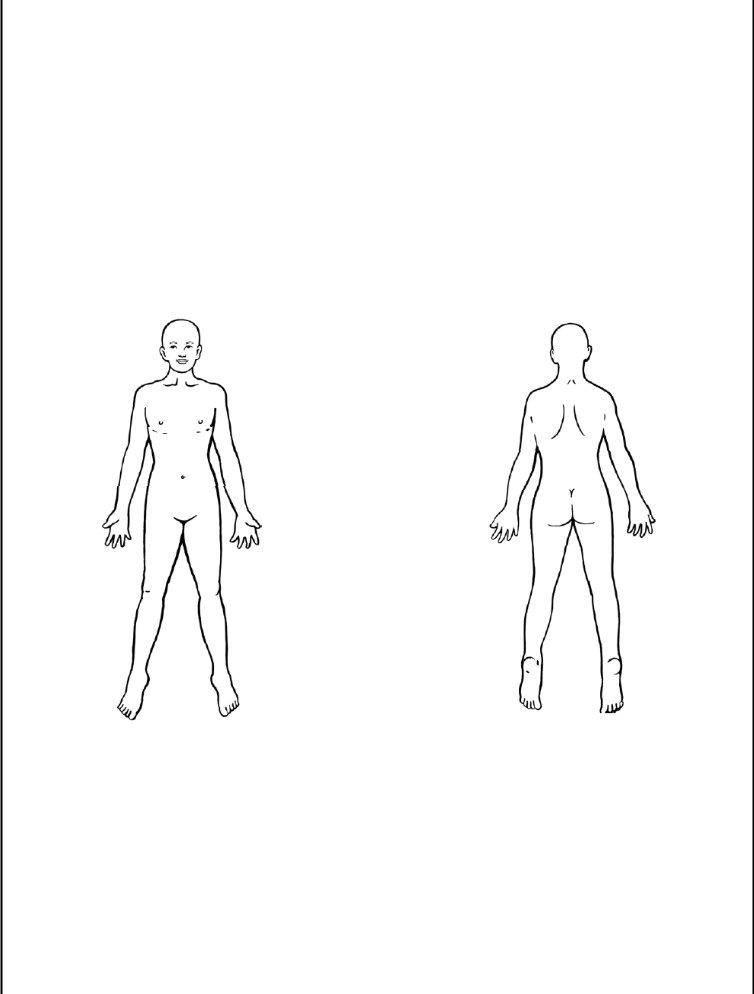
- Record all findings using diagrams, legend, and a consecutive numbering system. |
|
|
|
|
|
|
||||||||||||
|
|
- If injuries are described or if remarkable findings or possible trauma are observed, |
|
|
|
|
|
|
||||||||||||
|
|
please photograph. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
1a. Weight |
b. Blood |
Pressure |
c. Pulse |
|
d. Resp |
|
e. Temp |
f. Pulse Oxygen |
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
2a. Exam Started |
|
|
|
b. Exam Completed |
|
|
|
|
|
|
|
||||||||
|
Date (YYYYMMDD) |
|
Time |
Date (YYYYMMDD) |
Time |
|
Patient Identification |
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
3. Describe general physical appearance. |
4. Describe general demeanor. (Including affect, behavior |
|
5. Describe condition of clothing upon |
||||||||||||||||
|
|
(Use observations, not conclusions.) |
|
|
|
and orientation. Use observations, not conclusions.) |
|
|
arrival. (If the patient has not changed after |
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
the assault) |
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
6. Collect outer and underclothing if indicated. |
7. |
Conduct a physical examination. Use the history obtained earlier to guide your examination and recovery |
|||||||||||||||||
|
|
|
Not indicated |
|
|
|
|
|
|
of evidence. |
|
|
|
|
Findings |
|
No Findings Observed |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
8. Scan the entire body with an Alternate Light Source (such as a Wood's Lamp). Collect dried and moist secretions, stains, and foreign materials from the body.
Label box and envelope with the location of the collection. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Findings |
|
|
No Findings Observed |
||||||||||||
9. Was there a history of scratching? |
|
No |
|
|
Yes |
|
Unsure |
|
If yes or unsure, collect fingernail clippings. If there is not enough fingernail to clip, then swab |
|||||||||||||||||||||||
|
|
|
|
|||||||||||||||||||||||||||||
|
|
|
|
|
fingernails. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
10. Was there a history of kissing, licking or sucking parts of the body? |
|
No |
|
|
Yes |
|
|
Unsure |
|
|
|
|
|
|
||||||||||||||||||
|
If yes or unsure, collect swabs of the body areas that were believed to be contacted by the suspect's mouth. (Head and genitals are addressed in the next sections.) |
|||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Diagram A |
|
|
|
|
|
|
|
|
|
|
|
|
|
Diagram B |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
LEGEND: TYPES OF FINDINGS. RECORD ALL CLOTHING AND SPECIMENS COLLECTED IN SECTION O. |
|
|
||||||||||||||||||||||||||
AB |
Abrasion |
BU |
Burn |
DF |
Deformity |
FB |
Foreign Body |
MS |
Moist Secretion |
PE |
Petechiae |
|
SW |
Swelling |
||||||||||||||||||
ALS Alternate Light CS |
Control Swab |
DS |
Dry Secretion |
IN |
Induration |
OF |
Other Foreign |
PS |
Potential Saliva |
|
TB |
Toluidine Blue |
||||||||||||||||||||
|
Source |
CT |
Contusion (bruise) |
ER |
Erythema (redness) IW |
Incised Wound |
|
Materials (describe) |
SHX Sample Per History |
TE |
Tenderness |
|||||||||||||||||||||
BI |
Bite |
DE |
Debris |
F/H |
Fiber/Hair |
LA |
Laceration |
OI |
Other Injury |
(describe) |
SI |
Suction Injury |
|
V/S |
Vegetation/Soil |
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
Locator # |
|
Type |
|
|
|
Description |
|
|
|
Locator # |
Type |
|
|
|
|
|
|
Description |
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DD FORM 2911, SEP 2011 |
Page 6 of 14 Pages |
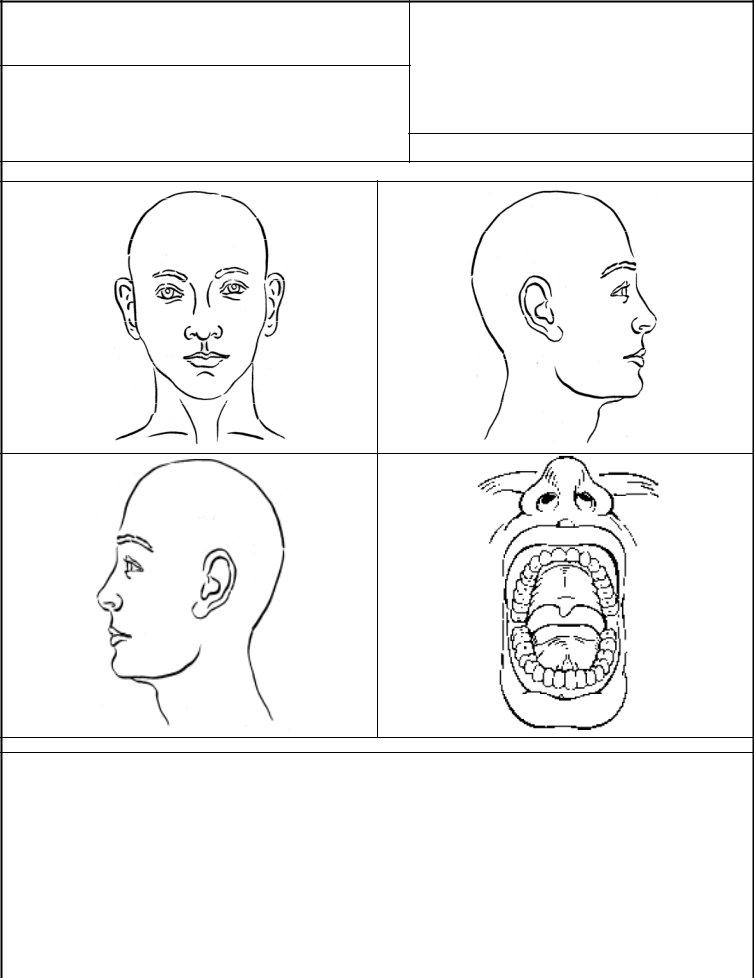
J.HEAD, NECK, THROAT AND ORAL EXAMINATION
-Record all findings, including tenderness and pain, using diagrams, legend, and a consecutive numbering system.
-If injuries are described or if remarkable findings or possible trauma are observed, please photograph.
1.Examine the face, head, hair, scalp, neck and throat for injury and foreign materials.
|
|
Findings |
|
No Findings Observed |
|
|
|
|
|
2.Collect dried and moist secretions, stains, and foreign materials from the face, head,
hair, neck, throat and scalp. |
|
Findings |
|
No Findings Observed |
|
|
|
|
|
3.Examine the oral cavity for injury and foreign material (If indicated by assault history).
Collect foreign materials.
Exam done: |
|
Not applicable |
|
Yes |
|
Findings |
|
No Findings Observed |
|
|
|
|
|
|
|
|
|
Patient Identification
4.Collect at a minimum 1 external mouth swab and 2 swabs from the oral cavity (if indicated by history).
5. Collect head hair combing or brushing.
Diagram C
Diagram D
Diagram E
Diagram F
LEGEND: TYPES OF FINDINGS. RECORD ALL SPECIMENS COLLECTED IN SECTION O.
AB |
Abrasion |
BU |
Burn |
DF |
Deformity |
FB |
Foreign Body |
MS |
Moist Secretion |
PE |
Petechiae |
SW |
Swelling |
||||
ALS Alternate Light CS |
Control Swab |
DS |
Dry Secretion |
IN |
Induration |
OF |
Other Foreign |
PS |
Potential Saliva |
TB |
Toluidine Blue |
||||||
|
Source |
CT |
Contusion (bruise) |
ER |
Erythema (redness) |
IW |
Incised Wound |
|
Materials (describe) |
SHX |
Sample Per History |
TE |
Tenderness |
||||
BI |
Bite |
DE |
Debris |
F/H |
Fiber/Hair |
LA |
Laceration |
OI |
Other Injury (describe) |
SI |
Suction Injury |
V/S |
Vegetation/Soil |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
Locator # |
|
Type |
|
|
Description |
|
|
Locator # |
Type |
|
|
Description |
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DD FORM 2911, SEP 2011 |
Page 7 of 14 Pages |
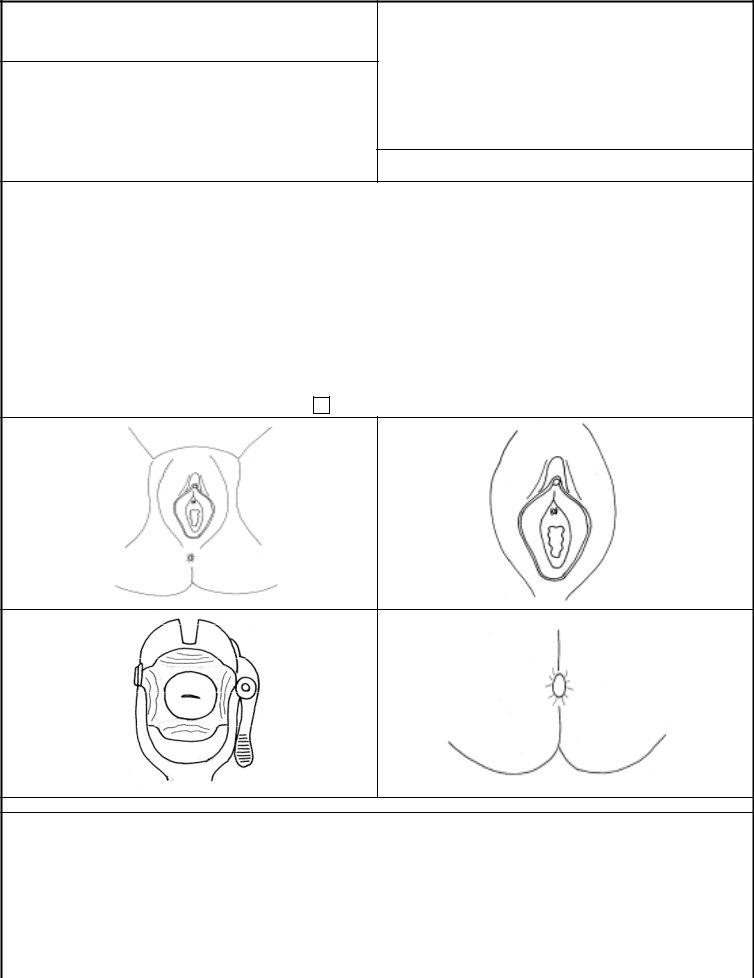
K.GENITAL EXAMINATION - FEMALE
-Record all findings, including tenderness and pain, using diagrams, legend, and a consecutive numbering system.
-If injuries are described or if remarkable findings or possible trauma are observed, please photograph.
1. Examine the inner thighs, external genitalia, and perineal area.
|
If there are findings, describe (including location). |
|
Findings |
|
No Findings |
|||
|
|
|||||||
. (If available and appropriate, consider the use of |
|
|
||||||
|
|
Observed |
||||||
|
toluidine blue dye.) |
Clitoral hood and |
|
|
|
|||
|
|
|
|
|
||||
|
|
Abdomen |
|
|
|
|
|
|
|
|
|
surrounding area |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Thighs |
|
Periurethral tissue/ |
|
|
|
|
|
|
|
urethral meatus |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Perineum |
|
Hymen |
|
|
|
|
|
|
Labia majora |
|
Fossa navicularis |
|
|
|
|
|
|
|
|
|
|
|
||
|
|
Labia minora |
|
Posterior fourchette |
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
Patient Identification
2. Scan the area with an Alternate Light Source. Collect dried and moist
secretions, stains, and foreign materials. |
|
Findings |
|
No Findings Observed |
|
|
|
|
|
3. Collect pubic hair combing or brushing. If there is no pubic hair, conduct an external swab of genitalia.
4. Examine the vagina and cervix. If there are findings, describe (including |
5. Examine the buttocks, anus, and perineum. |
|||||||||||
|
location). (If available and appropriate, consider the use of toluidine blue dye.). |
a. Findings from buttocks, anus, or perineum. If there are findings, describe |
||||||||||
|
|
|
|
|
||||||||
|
|
Findings |
|
No Findings Observed |
(including location) (If available and appropriate, consider use of toluidine blue dye.). |
|||||||
|
|
|
|
|
|
|
Yes |
|
No Findings Observed |
|
||
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
b. Collect dried and moist secretions, and foreign materials. |
|||||||
a. Collect the following swabs: 2 pubic mound (if there is no pubic hair), 2 vaginal, and |
|
|
Findings |
|
|
No Findings Observed |
||||||
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|||||
|
2 cervical. |
|
|
c. Collect 2 swabs of the perineum. |
d. Collect 2 anal swabs. |
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
6. Conduct a rectal exam (using anoscope if possible) if rectal injury is suspected or if there is any sign of rectal bleeding.
a. Rectal exam done: |
|
Yes |
|
Not applicable |
||
b. Rectal bleeding: |
|
No |
|
Yes |
|
|
|
|
|
|
|||
c. Was an anoscopic exam done? |
|
No |
|
Yes |
||
|
|
|||||
d. If exam was done, what position was used? |
|
Supine Lithotomy |
||||
|
||||||
e. If exam was done, describe findings: |
f. Collect a rectal swab if indicated. |
Other (describe)
Diagram G
Diagram H
Diagram I
Diagram J
LEGEND: TYPES OF FINDINGS. RECORD ALL SPECIMENS COLLECTED IN SECTION O.
AB |
Abrasion |
|
BU |
Burn |
DF |
Deformity |
FB |
Foreign Body |
MS |
Moist Secretion |
PE |
Petechiae |
SW |
Swelling |
||||
ALS Alternate Light |
CS Control Swab |
DS |
Dry Secretion |
IN |
Induration |
OF |
Other Foreign |
PS |
Potential Saliva |
TB |
Toluidine Blue |
|||||||
|
Source |
|
CT |
Contusion (bruise) |
ER |
Erythema (redness) |
IW |
Incised Wound |
|
Materials (describe) |
SHX |
Sample Per History |
TE |
Tenderness |
||||
BI |
Bite |
|
DE |
Debris |
F/H |
Fiber/Hair |
LA |
Laceration |
OI |
Other Injury (describe) |
SI |
Suction Injury |
V/S |
Vegetation/Soil |
||||
Locator # |
|
Type |
|
|
|
Description |
|
|
Locator # |
Type |
|
|
Description |
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DD FORM 2911, SEP 2011 |
Page 8 of 14 Pages |
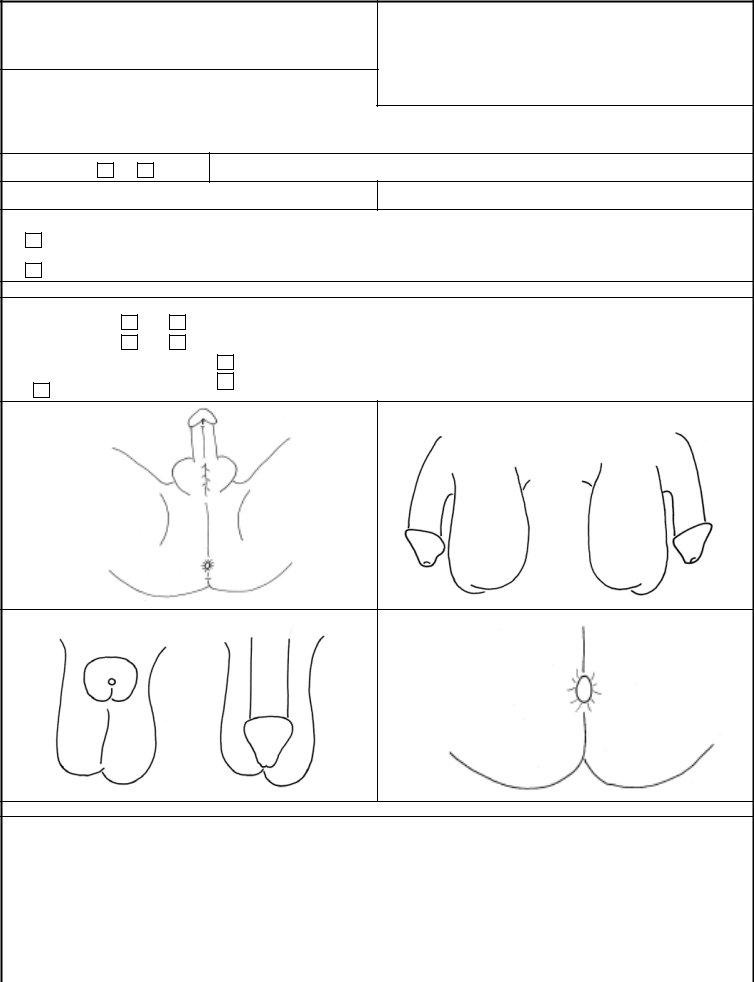
L.GENITAL EXAMINATION - MALE
-Record all findings, including tenderness and pain, using diagrams, legend, and a consecutive numbering system.
-If injuries are described or if remarkable findings or possible trauma are observed, please photograph.
1. Examine the inner thighs, external genitalia, and perineal area.
If there are findings, describe (including location). (If available and appropriate,
consider the use of toluidine blue dye.) |
|
|
Findings |
|
No Findings Observed |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
Abdomen |
|
Urethral meatus |
|
|
Glans |
|
|
|
|
|
Thighs |
|
Shaft |
|
|
|
|
||
|
|
|
|
|
|
|||||
|
|
|
|
|
Testes |
|
|
|||
|
|
|
|
|
|
|
||||
|
|
Foreskin |
|
Scrotum |
|
|
|
|
||
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
Patient Identification
2. Circumcised:
No
Yes
3. Scan the area with an Alternate Light Source (such as a Wood's Lamp). Collect dried and moist secretions,
stains, and foreign materials. |
|
Findings |
|
No Findings Observed |
|
|
|
|
|
|
|
4.Collect pubic hair combing or brushing. If no pubic hair, conduct external swab at base of penis.
5.If indicated by assault history, collect the following swabs: 2 penile and 2 scrotal.
6.Examine the buttocks and perineum (if indicated by history). a. Findings from buttocks, anus, or perineum.
Yes |
|
None Observed |
b. Collect dried and moist secretions, and foreign materials.
Findings |
|
No Findings Observed |
If there are findings, describe (including location). (If available and appropriate, consider the use of toluidine blue dye.)
7.Collect 2 anal swabs.
8.Conduct a rectal exam (using anoscope if possible) if rectal injury is suspected or if there is any sign of rectal bleeding.
a.Rectal exam done?
b.Rectal bleeding:
Yes
Yes
No |
e. If exam was done, describe findings: |
None Observed
c. Was an anoscopic exam done? |
|
Yes |
|
|
|
d. If exam was done, what position was used?
Other (describe)
No
Supine
Diagram K
Diagram L
Diagram M
Diagram N
LEGEND: TYPES OF FINDINGS. RECORD ALL SPECIMENS COLLECTED IN SECTION O.
AB |
Abrasion |
|
BU |
Burn |
DF |
Deformity |
FB |
Foreign Body |
MS |
Moist Secretion |
PE |
Petechiae |
SW |
Swelling |
||||
ALS Alternate Light |
CS Control Swab |
DS |
Dry Secretion |
IN |
Induration |
OF |
Other Foreign |
PS |
Potential Saliva |
TB |
Toluidine Blue |
|||||||
|
Source |
|
CT |
Contusion (bruise) |
ER |
Erythema (redness) |
IW |
Incised Wound |
|
Materials (describe) |
SHX |
Sample Per History |
TE |
Tenderness |
||||
BI |
Bite |
|
DE |
Debris |
F/H |
Fiber/Hair |
LA |
Laceration |
OI |
Other Injury (describe) |
SI |
Suction Injury |
V/S |
Vegetation/Soil |
||||
Locator # |
|
Type |
|
|
|
Description |
|
|
Locator # |
Type |
|
|
Description |
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DD FORM 2911, SEP 2011 |
Page 9 of 14 Pages |
M. TOXICOLOGY |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
Toxicology examples must be collected as soon as possible due to the |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||
limited time frame in which they can be collected. If the assault happened within |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||
96 hours of the examination and the answer to any of these questions is Yes or |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||
Unsure, use the DoD Toxicology Kit. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
1. |
Loss of memory? (If yes, describe) |
|
|
|
|
|
|
No |
|
|
Yes |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Patient Identification |
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
2. |
Lapse of consciousness? (If yes, describe) |
|
|
|
No |
|
Yes |
|
|
Unsure |
|
3. Vomited? (If yes, describe. Include location and number of |
|
No |
|
|
Yes |
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
times.) |
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
4.a. Voluntary ingestion of alcohol/drugs? |
|
|
|
No |
|
Yes |
|
|
Unsure |
|
b. Involuntary ingestion of alcohol/drugs? |
|
No |
|
Yes |
|
|
Unsure |
||||||||||||||||||||
|
If yes: |
|
|
Alcohol |
|
|
Drugs |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
If yes: |
|
Alcohol |
|
Drugs |
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
5. |
Was a clinical toxicology lab conducted? |
|
No |
|
|
Yes |
|
6. FOR UNRESTRICTED REPORTS: Was a DoD Toxicology Kit completed? |
|
No |
|
|
Yes |
|||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
N. RECORD EXAM METHODS |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
1. |
Direct visualization only |
|
|
No |
|
Yes |
5. |
Toluidine Blue Dye |
|
|
No |
|
|
(If Other, describe) |
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Yes |
|
|
|
|
|
|
|
|
|
|
|
|||||
2. |
Alternate Light Source |
|
|
No |
|
Yes |
|
6. Anoscopic exam |
|
|
No |
|
Yes |
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
3. |
Digital Camera |
|
|
|
|
|
No |
|
Yes |
|
7. Vaginal speculum exam |
|
|
No |
|
Yes |
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
4. |
Colposcope or Other Magnifier |
|
|
No |
|
Yes |
|
8. Other |
|
|
|
|
|
|
No |
|
Yes |
|
|
|
|
|
|
|
|
|
|
|
||||||||||
O. OBSERVATIONS. Please describe your observations.
DD FORM 2911, SEP 2011 |
Page 10 of 14 Pages |
P. EVIDENCE COLLECTED |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
No |
|
|
Yes |
Time Completed |
|
|
|
|
|
|
|
|
|
1. |
TOXICOLOGY KIT |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Completed By |
|
|
|
|
|
Released To |
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Patient Identification |
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
2. |
CLOTHING |
|
|
|
|
No |
|
|
Yes |
Time Completed |
|
Completed By |
|
|
|
Released To |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
a. Undergarments placed in evidence kit |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
b. Clothing placed in bags |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3. |
OTHER: |
|
|
|
|
No |
|
|
Yes |
Time Completed |
|
Completed By |
|
|
|
Released To |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
a. |
Swabs, suspected blood |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
b. |
Dried secretions |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
c. |
Fiber/loose hairs |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
d. |
Vegetation |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
e. |
Soil/debris |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
f. |
Swabs/suspected semen |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
g. Swabs/suspected saliva |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
h. Swabs/Alternate Light Source area(s) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
i. |
Fingernail cuttings |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
j. |
Fingernail scrapings/swabbings |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
k. |
Matted hair cuttings |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
l. |
Pubic hair combings/brushings |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
m. Intravaginal foreign body (If yes, describe) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
n. Other types (If yes, describe) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4. ORAL, GENITAL, RECTAL SAMPLES |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
# Swabs |
Time Completed |
|
|
|
Completed By |
|
|
# Swabs |
Time Completed |
|
Completed By |
||||||||
a. External oral swab(s) |
|
|
|
|
|
|
|
|
|
|
|
f. |
Perineal swab(s) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
b. Oral cavity swab(s) |
|
|
|
|
|
|
|
|
|
|
|
g. |
Anal swab(s) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
c. Vaginal swab(s) |
|
|
|
|
|
|
|
|
|
|
|
h. |
Rectal swab(s) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
i. |
Other |
|
|
|
|
|
|
|
d. Cervical swab(s) |
|
|
|
|
|
|
|
|
|
|
|
|
(If yes, describe) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
e. Pubic mound swab(s) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
5. REFERENCE SAMPLES |
|
No |
Yes |
Time Completed |
|
Completed By |
|
|
|
No |
Yes |
Time Completed |
Completed By |
||||||||
a. Blood Card |
|
|
|
|
|
|
|
|
|
|
d. Other (describe) |
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
b. Known Head Hair |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
c. Known Pubic Hair |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DD FORM 2911, SEP 2011 |
Page 11 of 14 Pages |

Q. PHOTO DOCUMENTATION METHODS |
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
1. |
TYPE OF CAMERA |
|
|
|
|
|
|
|
|
|
|
|
|
35 mm |
Polaroid |
Digital |
Colposcope |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
Other |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2. |
DISPOSITION OF FILM/DISK |
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
Patient Identification |
|||
3. |
PHOTO LIST |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
Photo Number |
|
|
|
Description of Photo |
|
|
|
|
||||
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
R. OTHER DOCUMENTS INCLUDED - If there are any other documents included with this report, please list: |
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
S. PERSONNEL INVOLVED - Print names. |
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
||
1. |
HISTORY TAKEN BY |
|
Telephone (Include Area Code) |
2. EXAM PERFORMED BY |
|
|
|
Telephone (Include Area Code) |
||||
|
|
|
|
|
|
|
|
|
|
|||
3. |
SPECIMENS LABELED AND SEALED BY |
Telephone (Include Area Code) |
4. ASSISTED BY |
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
||
T. EVIDENCE DISTRIBUTION |
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
1. |
TOXICOLOGY KIT GIVEN TO: |
|
|
2. |
EVIDENCE KIT AND |
|
|
BAGS GIVEN TO: |
||||
|
|
|
|
|
|
|
|
|
|
|||
3. |
ITEMS RETURNED TO PATIENT (describe) |
|
4. |
OTHER (describe) |
|
|
|
|
||||
|
|
|
|
|
|
|
Given to: |
|
|
|
|
|
U. PERSON RECEIVING EVIDENCE - For Unrestricted Report - MCIO; for Restricted Report - See Service Policy. |
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
1. |
SIGNATURE |
|
|
|
2. |
PRINTED NAME AND ID NUMBER |
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
3. |
AGENCY |
|
|
|
4. |
DATE (YYYYMMDD) |
|
|
5. TELEPHONE (Include Area Code) |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
DD FORM 2911, SEP 2011 |
Page 12 of 14 Pages |
DoD SEXUAL ASSAULT FORENSIC EXAMINATION REPORT
PART II - DoD TOXICOLOGY KIT - FOR UNRESTRICTED REPORTS ONLY
BLOOD AND URINE SPECIMEN COLLECTION INSTRUCTIONS
Notes:
(A)This kit is to be used in conjunction with a DoD Medical Forensic Examination Kit when the patient indicates that there was memory loss, lapse of consciousness, involuntary or voluntary ingestion of drugs or alcohol, or if toxicology testing is otherwise indicated.
(B)Collect both blood and urine specimens in all cases.
(C)Urine samples should be collected from the victim as soon as possible due to the short window of detection for many of the drugs (including alcohol) involved in sexual assault.
(D)Based on timing of evidence pick up, refrigerate the sealed kit. However, if you are in a deployed or natural disaster environment that does not have refrigeration, it will be unlikely to preserve specimen.
STEP 1: Fill out the information requested on the Victim Information Form (next page).
BLOOD SPECIMEN COLLECTION
Note: Blood specimen collection must be performed only by a physician, registered nurse or trained phlebotomist.
STEP 2: Cleanse the blood collection site with the
Notes:
(A)Immediately after blood collection, assure proper mixing of anticoagulant powder by slowly and completely inverting the blood tube at least five times. Do NOT shake!
(B)Discard venipuncture needle(s) and prep pads as recommended by OSHA guidelines. Do NOT place the venipuncture needle(s) or prep pads in the specimen collection box.
STEP 3: Fill out all information requested on two of the three Specimen Security Seals provided. Then remove backing from the two Specimen Seals. Affix center of seals to the blood tube rubber stoppers, and press ends of seals down sides of the blood tubes, then place both filled and sealed blood tubes in specimen holder.
URINE SPECIMEN COLLECTION
STEP 4: Have subject void directly into the urine specimen bottle provided. A minimum of 60 ml is required.
STEP 5: After specimen is collected, replace cap and tighten down to prevent leakage.
STEP 6: Fill out the information requested on the remaining Specimen Security Seal. Affix center of seal to the bottle cap and press ends of seal down sides of bottle, then place urine bottle in specimen holder.
STEP 7: Place specimen holder inside the zip lock bag, then squeeze out excess air and close the bag. Place specimen holder in kit box.
Note: Do not remove liquid absorbing sheet from specimen bag.
STEP 8: Place DoD Toxicology Kit Victim Information form in Toxicology Kit. Retain a copy of the form with the SAFE Report.
STEP 9: Close kit box and affix kit box shipping seal where indicated.
STEP 10: Fill out all information requested on kit box top under "For Hospital Personnel".
STEP 11: Hand sealed kit to investigating agent.
Note: If the officer is not present at this time, place sealed kit in secure and refrigerated area, and hold for pickup by investigating officer. Work with law enforcement/investigating agent to ensure the CHAIN OF CUSTODY IS MAINTAINED.
MCIO or investigating agent should mail kit with Form 1323, Toxicological Request Form (found at: www.afip.org) to:
Armed Forces Medical Examiner
Division of Forensic Toxicology
Bldg 1102
1413 Research Boulevard
Rockville, MD 20850
EFFECTIVE 1 DEC 2011:
Armed Forces Medical Examiner
Division of Forensic Toxicology
Bldg 115
Purple Heart Drive
Dover AFB, DE 19902
DD FORM 2911, SEP 2011 |
Page 13 of 14 Pages |
DoD TOXICOLOGY KIT
VICTIM INFORMATION FORM
FOR UNRESTRICTED REPORTS ONLY
Patient Identification
1. |
VICTIM'S NAME (Last, First, Middle Initial) |
|
|
|
|||
|
|
|
|
|
|
|
|
2. |
VICTIM'S DATE OF BIRTH (YYYY/MM/DD) |
|
|
|
|||
|
|
|
|
|
|
|
|
3a. DATE OF SPECIMEN COLLECTION (YYYY/MM/DD) |
|
b. TIME |
|||||
|
|
|
|
|
|
|
|
4. |
IS VICTIM A SMOKER? |
|
|
|
|||
|
|
Yes |
|
No |
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
5. |
IS VICTIM TAKING ANY PRESCRIPTION DRUGS? |
|
|
|
|||
|
|
Yes |
|
No |
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
a. IF YES, NAME OF DRUG(S) |
|
|
|
||||
|
|
|
|
||||
b. DATE DRUG(S) LAST TAKEN (YYYY/MM/DD) |
|
c. TIME |
|||||
|
|
|
|
|
|||
6. |
IS VICTIM TAKING ANY |
|
|
||||
|
|
Yes |
|
No |
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
a. IF YES, NAME OF DRUG(S) |
|
|
|
||||
|
|
|
|
||||
b. DATE DRUG(S) LAST TAKEN (YYYY/MM/DD) |
|
c. TIME |
|||||
|
|
|
|
|
|||
7. |
WHY IS DRUG SCREEN BEING REQUESTED? |
|
|
|
|||
|
|
|
|
|
|||
8. |
PERSON COLLECTING SAMPLE |
|
|
|
|||
|
|
|
|
||||
a. NAME (Last, First, Middle Initial) |
b. TITLE |
|
c. DATE (YYYY/MM/DD) |
||||
|
|
|
|
|
|
|
|
DD FORM 2911, SEP 2011 |
COPY 1 - TO BE SENT WITH KIT TO AFIP |
Page 14 of 14 Pages |
DoD TOXICOLOGY KIT
VICTIM INFORMATION FORM
FOR UNRESTRICTED REPORTS ONLY
Patient Identification
1. |
VICTIM'S NAME (Last, First, Middle Initial) |
|
|
|
|||
|
|
|
|
|
|
|
|
2. |
VICTIM'S DATE OF BIRTH (YYYY/MM/DD) |
|
|
|
|||
|
|
|
|
|
|
|
|
3a. DATE OF SPECIMEN COLLECTION (YYYY/MM/DD) |
|
b. TIME |
|||||
|
|
|
|
|
|
|
|
4. |
IS VICTIM A SMOKER? |
|
|
|
|||
|
|
Yes |
|
No |
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
5. |
IS VICTIM TAKING ANY PRESCRIPTION DRUGS? |
|
|
|
|||
|
|
Yes |
|
No |
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
a. IF YES, NAME OF DRUG(S) |
|
|
|
||||
|
|
|
|
||||
b. DATE DRUG(S) LAST TAKEN (YYYY/MM/DD) |
|
c. TIME |
|||||
|
|
|
|
|
|||
6. |
IS VICTIM TAKING ANY |
|
|
||||
|
|
Yes |
|
No |
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
a. IF YES, NAME OF DRUG(S) |
|
|
|
||||
|
|
|
|
||||
b. DATE DRUG(S) LAST TAKEN (YYYY/MM/DD) |
|
c. TIME |
|||||
|
|
|
|
|
|||
7. |
WHY IS DRUG SCREEN BEING REQUESTED? |
|
|
|
|||
|
|
|
|
|
|||
8. |
PERSON COLLECTING SAMPLE |
|
|
|
|||
|
|
|
|
||||
a. NAME (Last, First, Middle Initial) |
b. TITLE |
|
c. DATE (YYYY/MM/DD) |
||||
|
|
|
|
|
|
|
|
DD FORM 2911, SEP 2011 |
COPY 2 - TO BE MAINTAINED WITH SAFE REPORT |
Page 14 of 14 Pages |