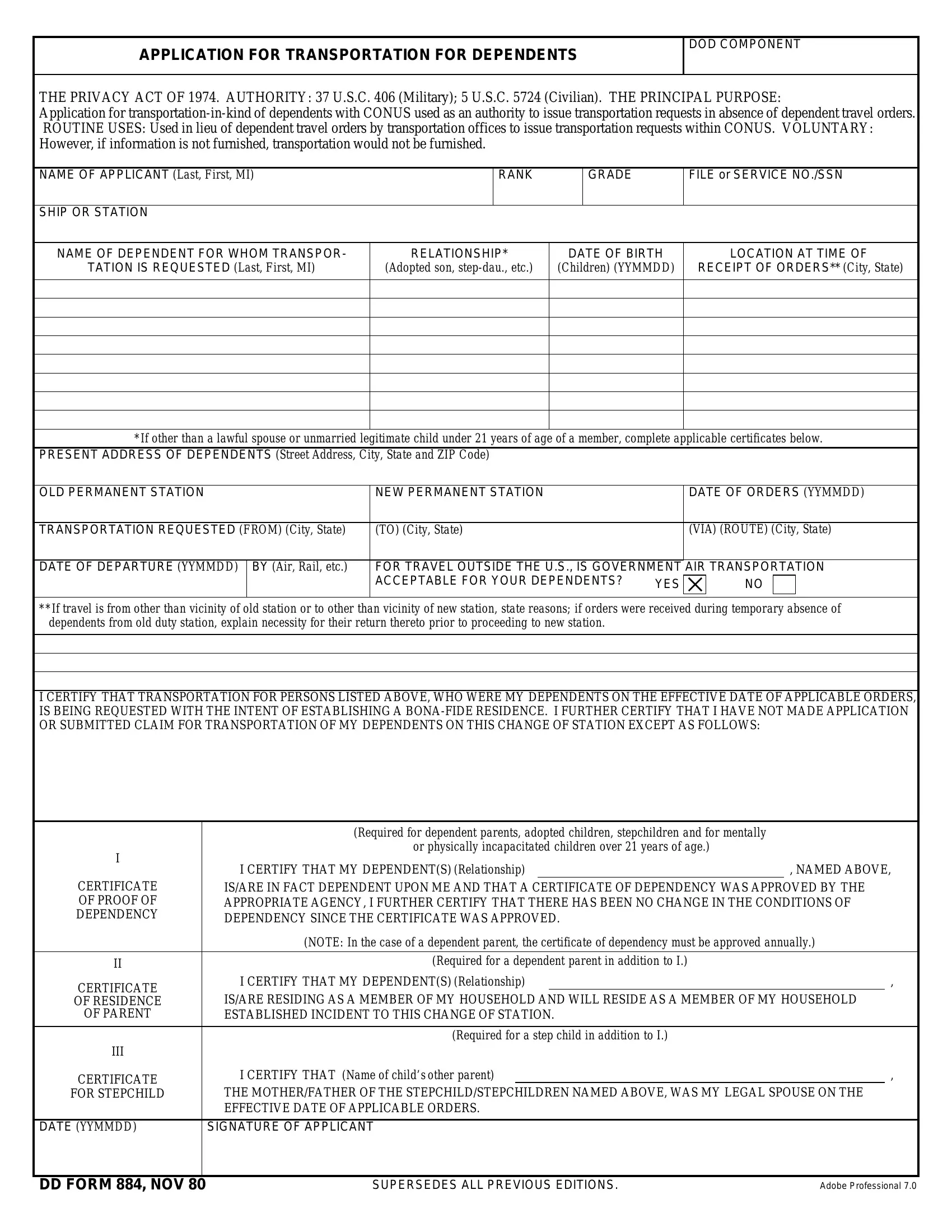
At the heart of facilitating the movement of military and civilian personnel's families across the United States lies the DD Form 884, known as the Application for Transportation for Dependents. Designed under the governance of The Privacy Act of 1974, this form serves dual vital roles. Firstly, it acts as an authoritative document for issuing transportation requests in the absence of dependent travel orders within the Continental United States (CONUS). Secondly, its structure is tailored to gather essential details regarding the applicant, such as their name, rank, and the dependents for whom transportation is requested, including their relationship to the applicant, date of birth, and current location. The form intricately outlines the specifics of the transportation needed, from the departure point to the destination, including the preferred route and mode of travel. Furthermore, the DD 884 form addresses various situations, such as dependent travel outside the U.S., and provides sections for certifying the dependency status of non-traditional dependents like stepchildren or dependents over the age of 21 with incapacities. The voluntary submission of this form is crucial; lack of information could result in the non-provision of transportation, emphasizing the form's significance in ensuring family members can join or accompany military and civilian personnel during station changes or similar transitions.
| Question | Answer |
|---|---|
| Form Name | Dd Form 884 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | CONUS, usnavy application form, navy form, 1974 |
APPLICATION FOR TRANSPORTATION FOR DEPENDENTS
DOD COMPONENT
THE PRIVACY ACT OF 1974. AUTHORITY: 37 U.S.C. 406 (Military); 5 U.S.C. 5724 (Civilian). THE PRINCIPAL PURPOSE:
Application for
NAME OF APPLICANT (Last, First, MI)
RANK
GRADE
FILE or SERVICE NO./SSN
SHIP OR STATION
NAME OF DEPENDENT FOR WHOM TRANSPOR-
TATION IS REQUESTED (Last, First, MI)
RELATIONSHIP*
(Adopted son,
DATE OF BIRTH
(Children) (YYMMDD)
LOCATION AT TIME OF
RECEIPT OF ORDERS** (City, State)
*If other than a lawful spouse or unmarried legitimate child under 21 years of age of a member, complete applicable certificates below.
PRESENT ADDRESS OF DEPENDENTS (Street Address, City, State and ZIP Code)
OLD PERMANENT STATION |
NEW PERMANENT STATION |
|
DATE OF ORDERS (YYMMDD) |
||||
|
|
|
|
|
|
|
|
TRANSPORTATION REQUESTED (FROM) (City, State) |
(TO) (City, State) |
|
(VIA) (ROUTE) (City, State) |
||||
|
|
|
|
|
|
|
|
DATE OF DEPARTURE (YYMMDD) |
BY (Air, Rail, etc.) |
FOR TRAVEL OUTSIDE THE U.S., IS GOVERNMENT |
AIR TRANSPORTATION |
||||
|
|
ACCEPTABLE FOR YOUR DEPENDENTS? |
YES |
|
NO |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
**If travel is from other than vicinity of old station or to other than vicinity of new station, state reasons; if orders were received during temporary absence of dependents from old duty station, explain necessity for their return thereto prior to proceeding to new station.
I CERTIFY THAT TRANSPORTATION FOR PERSONS LISTED ABOVE, WHO WERE MY DEPENDENTS ON THE EFFECTIVE DATE OF APPLICABLE ORDERS, IS BEING REQUESTED WITH THE INTENT OF ESTABLISHING A
|
(Required for dependent parents, adopted children, stepchildren and for mentally |
|
|
||||
I |
or physically incapacitated children over 21 years of age.) |
|
|
||||
I CERTIFY THAT MY DEPENDENT(S) (Relationship) |
|
, NAMED ABOVE, |
|||||
|
|||||||
CERTIFICATE |
IS/ARE IN FACT DEPENDENT UPON ME AND THAT A CERTIFICATE OF DEPENDENCY WAS APPROVED BY THE |
||||||
OF PROOF OF |
APPROPRIATE AGENCY, I FURTHER CERTIFY THAT THERE HAS BEEN NO CHANGE IN THE CONDITIONS OF |
||||||
DEPENDENCY |
DEPENDENCY SINCE THE CERTIFICATE WAS APPROVED. |
|
|
||||
|
|
|
|||||
|
(NOTE: In the case of a dependent parent, the certificate of dependency must be approved annually.) |
||||||
|
|
|
|
|
|
||
II |
(Required for a dependent parent in addition to I.) |
|
|
||||
CERTIFICATE |
I CERTIFY THAT MY DEPENDENT(S) (Relationship) |
|
|
, |
|||
OF RESIDENCE |
IS/ARE RESIDING AS A MEMBER OF MY HOUSEHOLD AND WILL RESIDE AS A MEMBER OF MY HOUSEHOLD |
||||||
OF PARENT |
ESTABLISHED INCIDENT TO THIS CHANGE OF STATION. |
|
|
||||
|
|
|
|
|
|||
|
(Required for a step child in addition to I.) |
|
|
||||
III |
|
|
|
|
|
|
|
CERTIFICATE |
I CERTIFY THAT (Name of child’s other parent) |
|
|
, |
|||
FOR STEPCHILD |
THE MOTHER/FATHER OF THE STEPCHILD/STEPCHILDREN NAMED ABOVE, WAS MY LEGAL SPOUSE ON THE |
||||||
|
EFFECTIVE DATE OF APPLICABLE ORDERS. |
|
|
||||
|
|
|
|
||||
DATE (YYMMDD) |
SIGNATURE OF APPLICANT |
|
|
||||
|
|
|
|
|
|
|
|
DD FORM 884, NOV 80 |
SUPERSEDES ALL PREVIOUS EDITIONS. |
Adobe Professional 7.0 |