EDD Form DE 2501 is a standardized document issued by California’s Employment Development Department (EDD). It is an application for Disability Insurance (DI) benefits, allowing eligible individuals to claim financial assistance when they cannot work due to a non-work-related illness, injury, pregnancy, or childbirth.
Completing the DE 2501 form is the initial step in applying for DI benefits, requiring applicants to provide detailed information about their medical condition, employment history, and other relevant details. Once submitted to the EDD, the DE 2501 form undergoes review to determine the applicant’s eligibility for disability benefits, with approved individuals receiving financial support to help cover their lost wages during their period of disability.
Other California Forms
There are more fillable California forms accessible with our editor. Just below, we selected several of the more popular PDFs under this category. Moreover, keep in mind that you can easily upload, fill out, and edit any PDF document at FormsPal.
Following the California Code of Regulations, Title 22, sections 1085, 1088, and 1326, the Social Security details must be disclosed. Read the data on the collection and maintenance of the data.
Here is a list of steps to fill out EDD Form DE 2501 required by law:
1. Put in the name and the Social Security number.
Identify the claimer’s Social Security number and input the legal name.
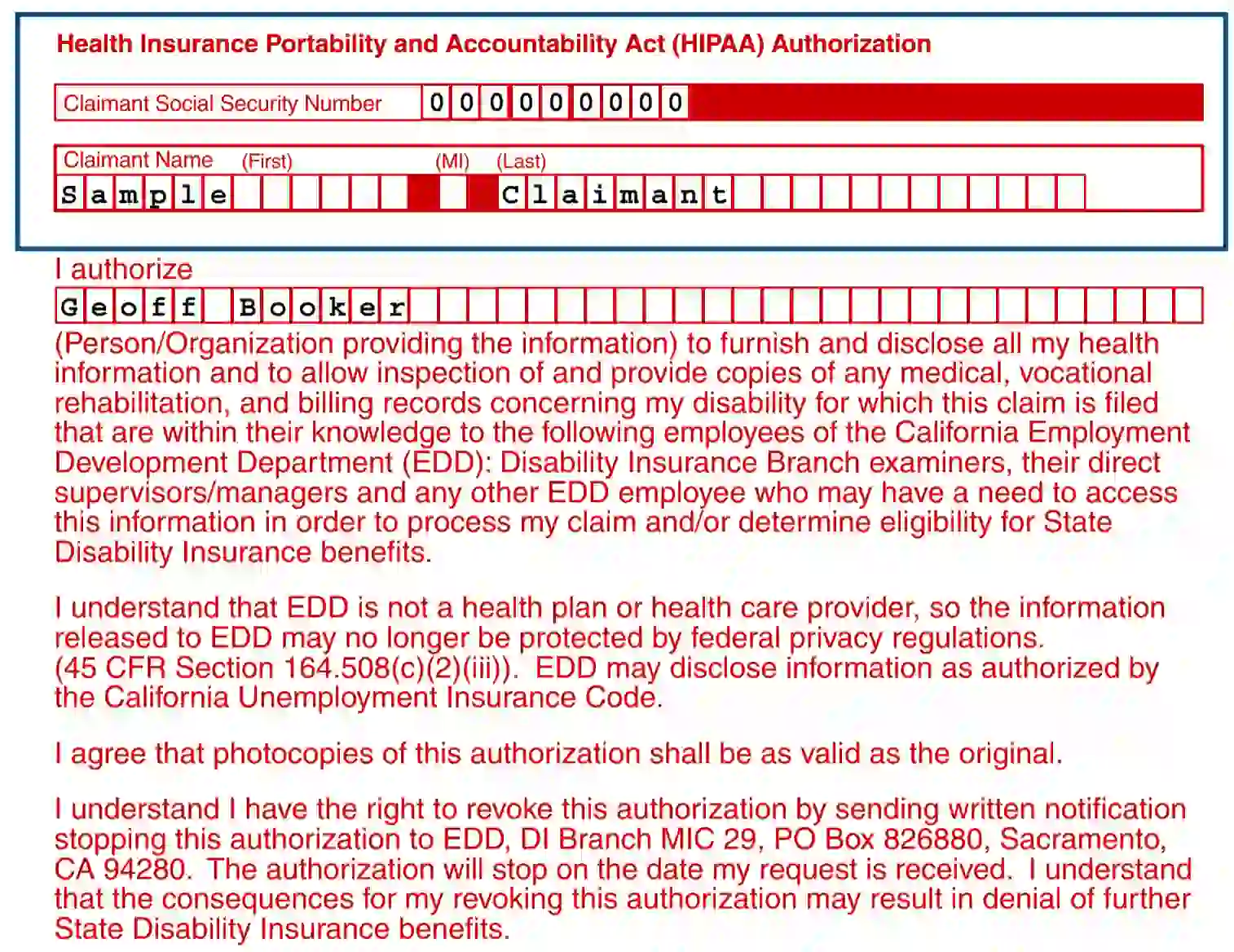
2. Authorize the person in charge
Input the info regarding the person to deal with any health-related data regarding the disability concerned. Ensure to read the following text in the body of the form to fully understand the procedure and the viable results.
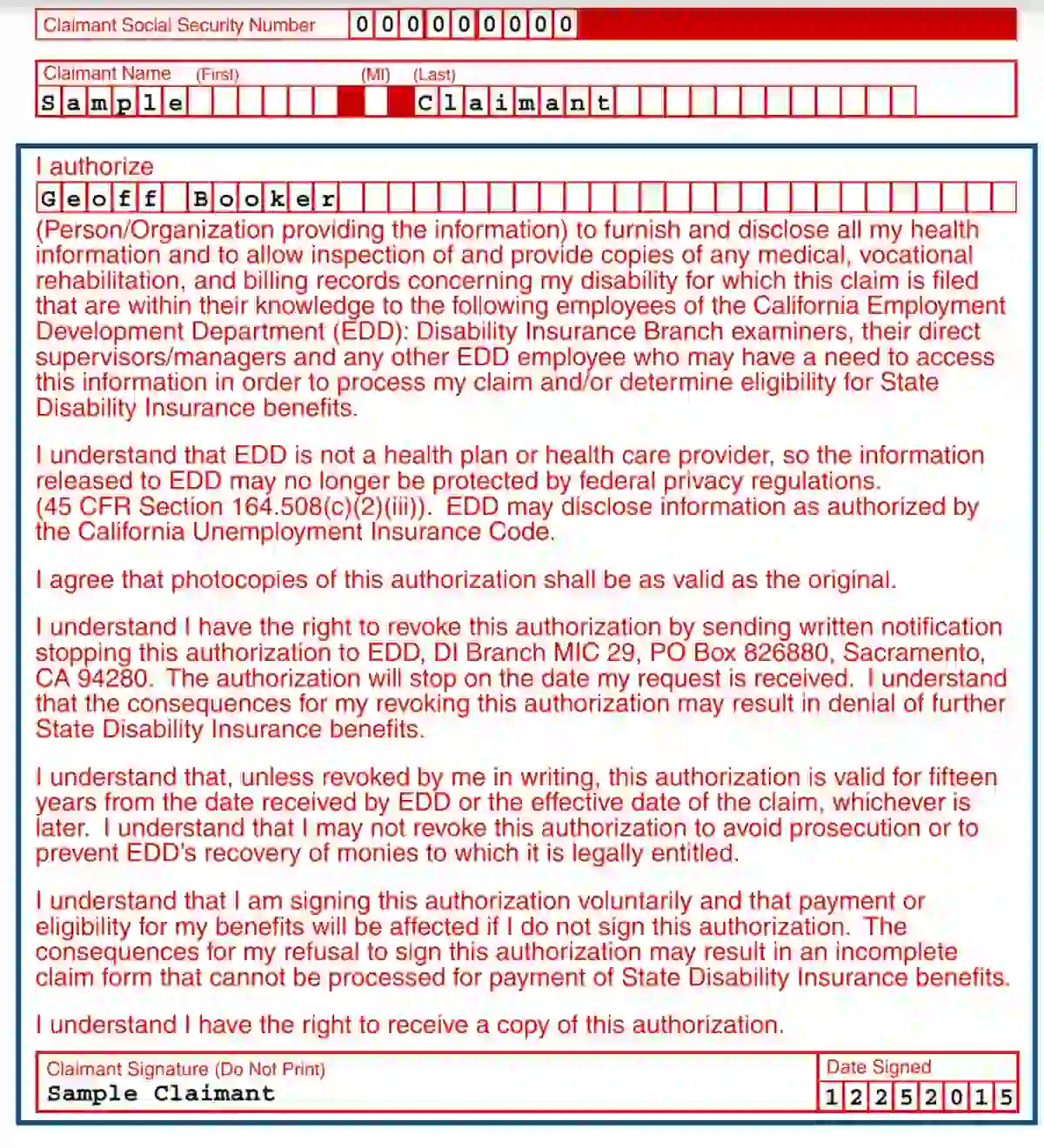
3. Put a sign and date
4. Fill out Part A
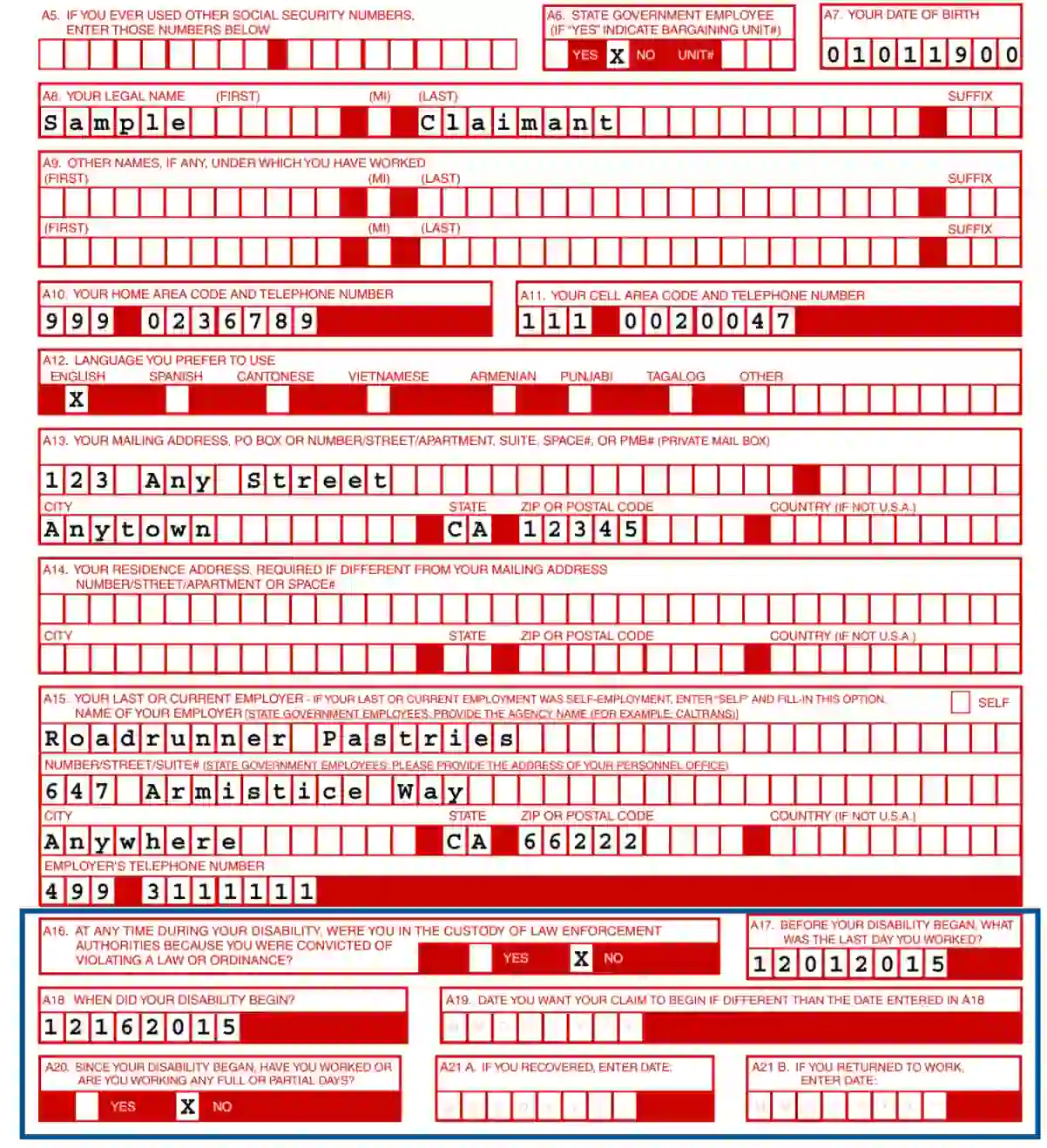
Fill out boxes A1—A13:
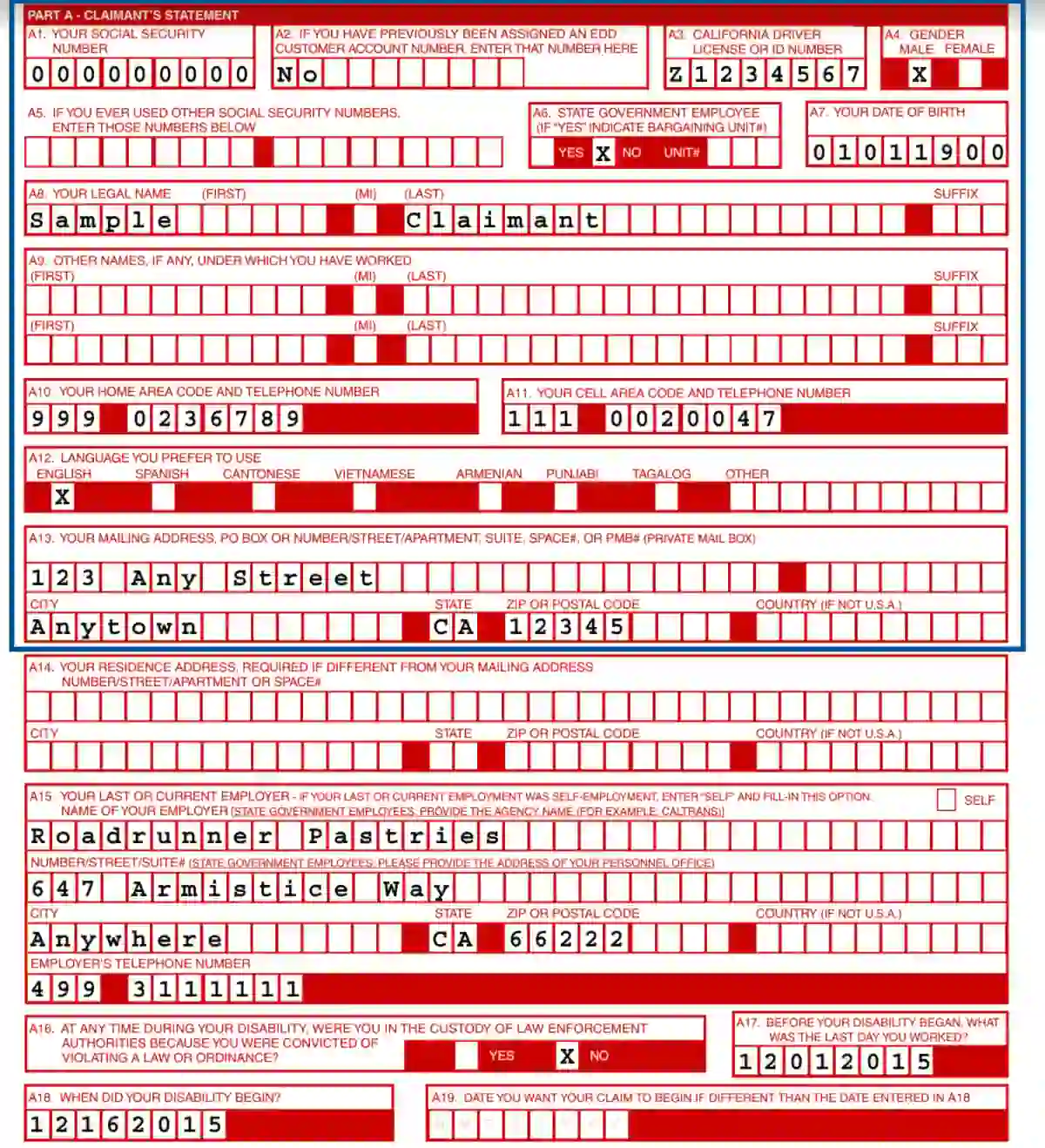
5. Identify the employer
Input information about the actual or previous employer

6. Provide more info
In A 16—A 21, put the date of the start of the illness, the last day you worked before the injury, the preferable date of the claim, information about full or partial shifts since the start of the disability, and the date of your return to work.
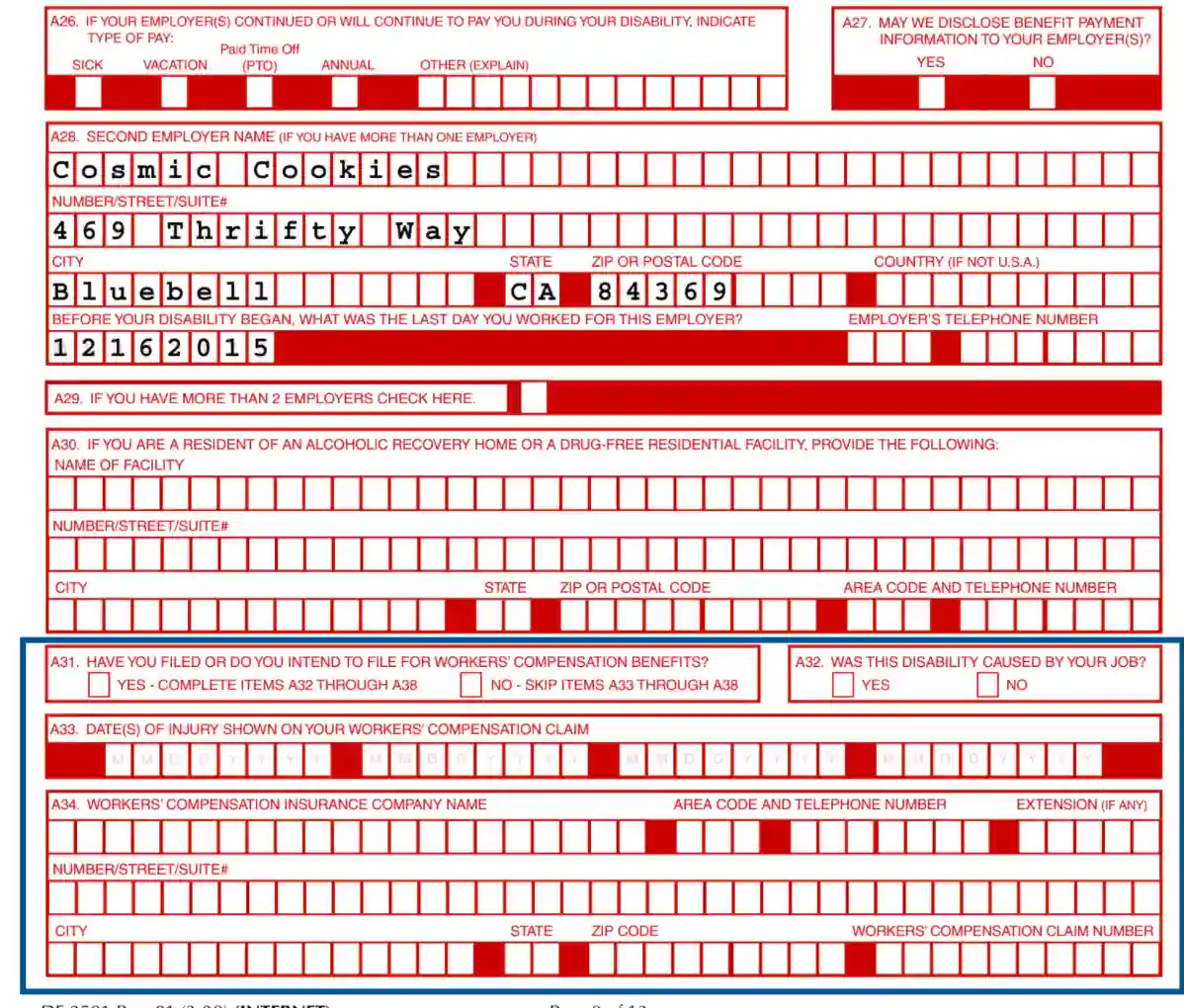
7. Reenter the Social Security code. Also, in sections A22— A27 provide the info about:

8. Provide info about the second employer and check the required box in A29

9. Provide the info about your residentship in a facility for alcohol and drug addiction recovery

10. Indicate if you have dealt with the claims before and verify if the disability is job-related; put in the date of injury and the insurance company title.
11. Input the Adjuster’s name
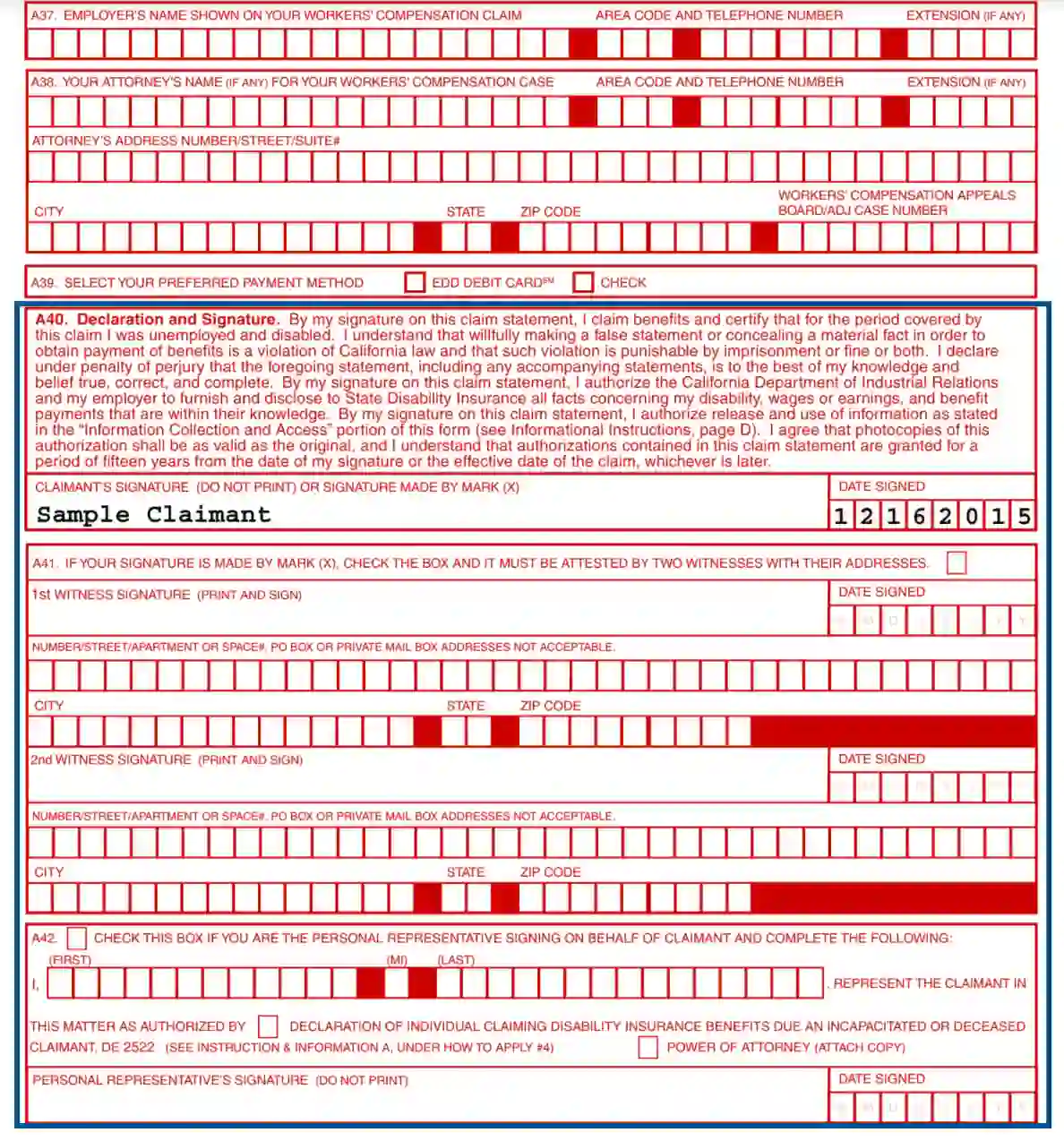
Do it after reentering your Social Security number and provide the info about the employer and attorney. All that and payment method is indicated in sections A35— A39.
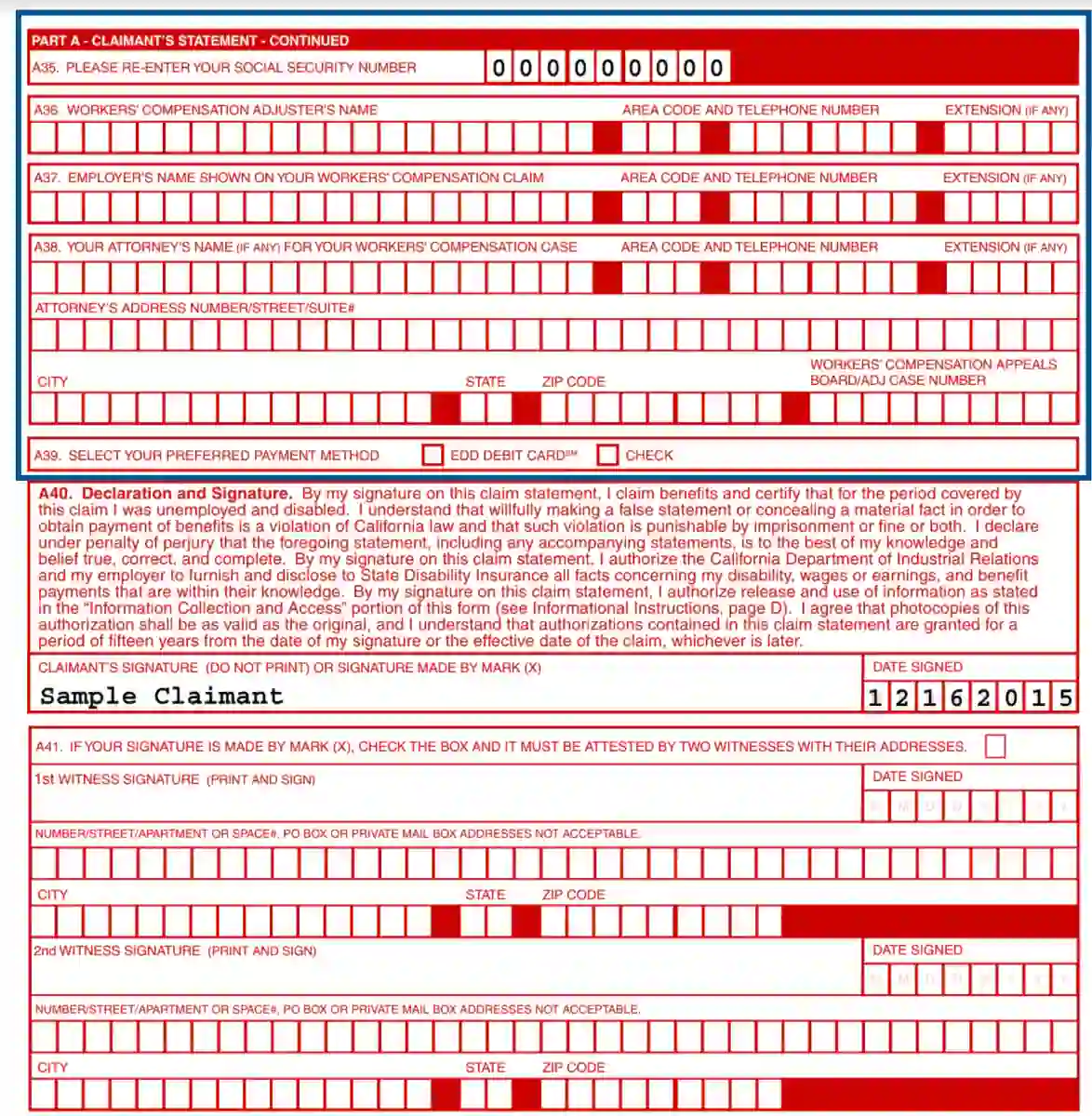
12. In sections A40— A 42, provide your and the witnesses’ signatures.
13. Have Part B filled out and signed by a physician.
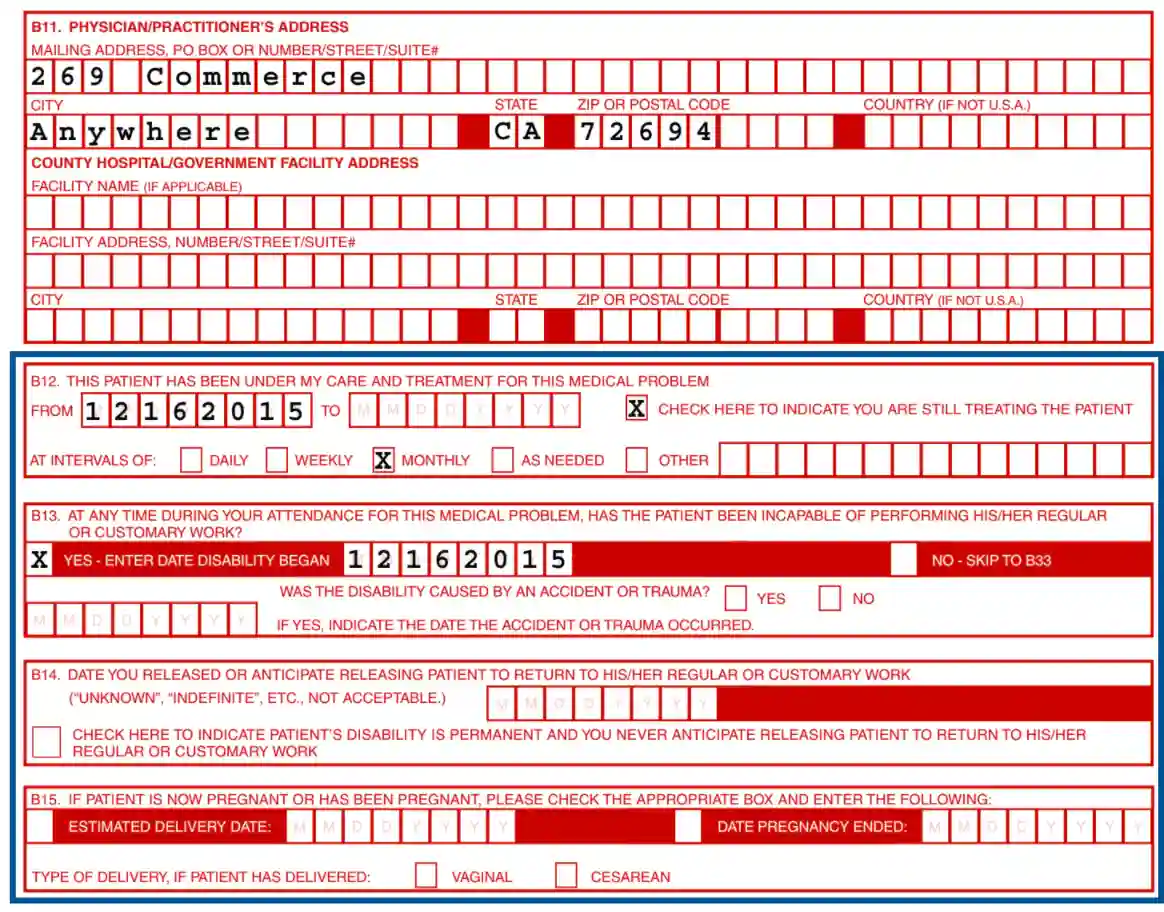
In sections B1—B11, you should fill out the information about the name, address, and phone number of the practitioner in charge of the injury.

14. Provide the time of the treatment, release, pregnancy details in B12—B15
15. In sections B16—B19, provide information about the patient’s release, abnormal pregnancy, and ICD diagnosis.
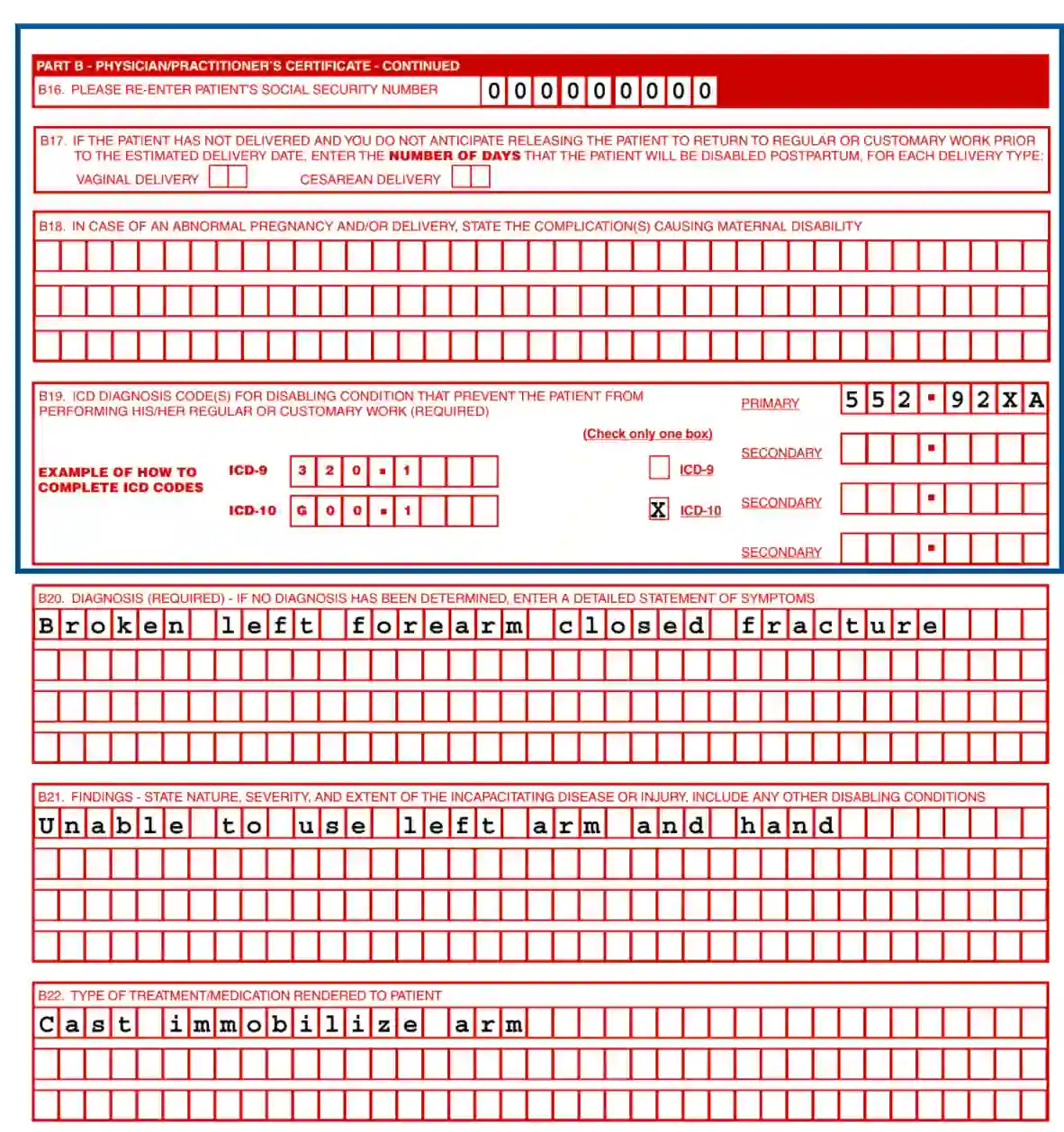
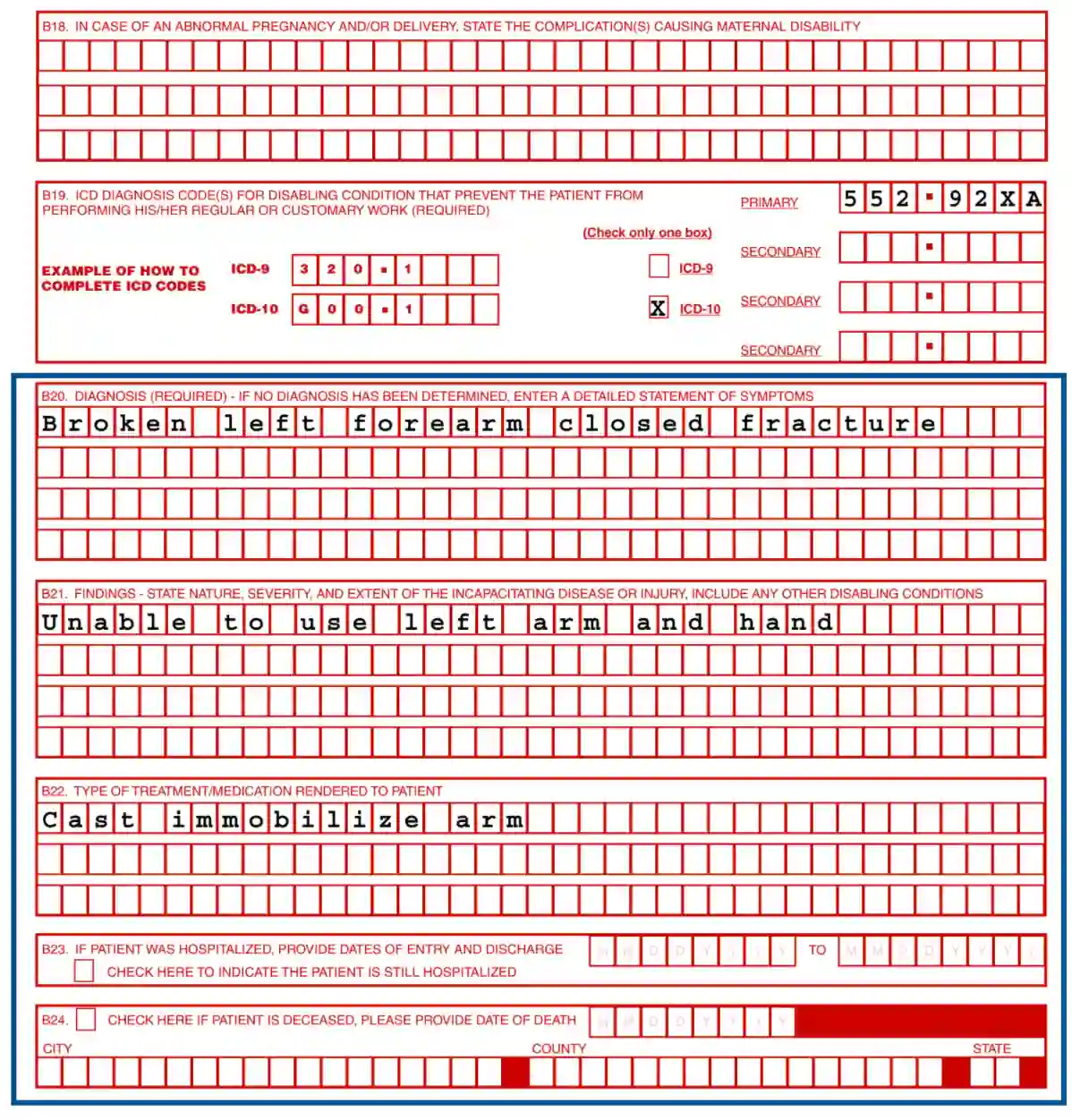
16. Input information about a diagnosis, findings, and treatment information
Also, add the date of the hospital entry and release or death of the patient in boxes B 20—B24.
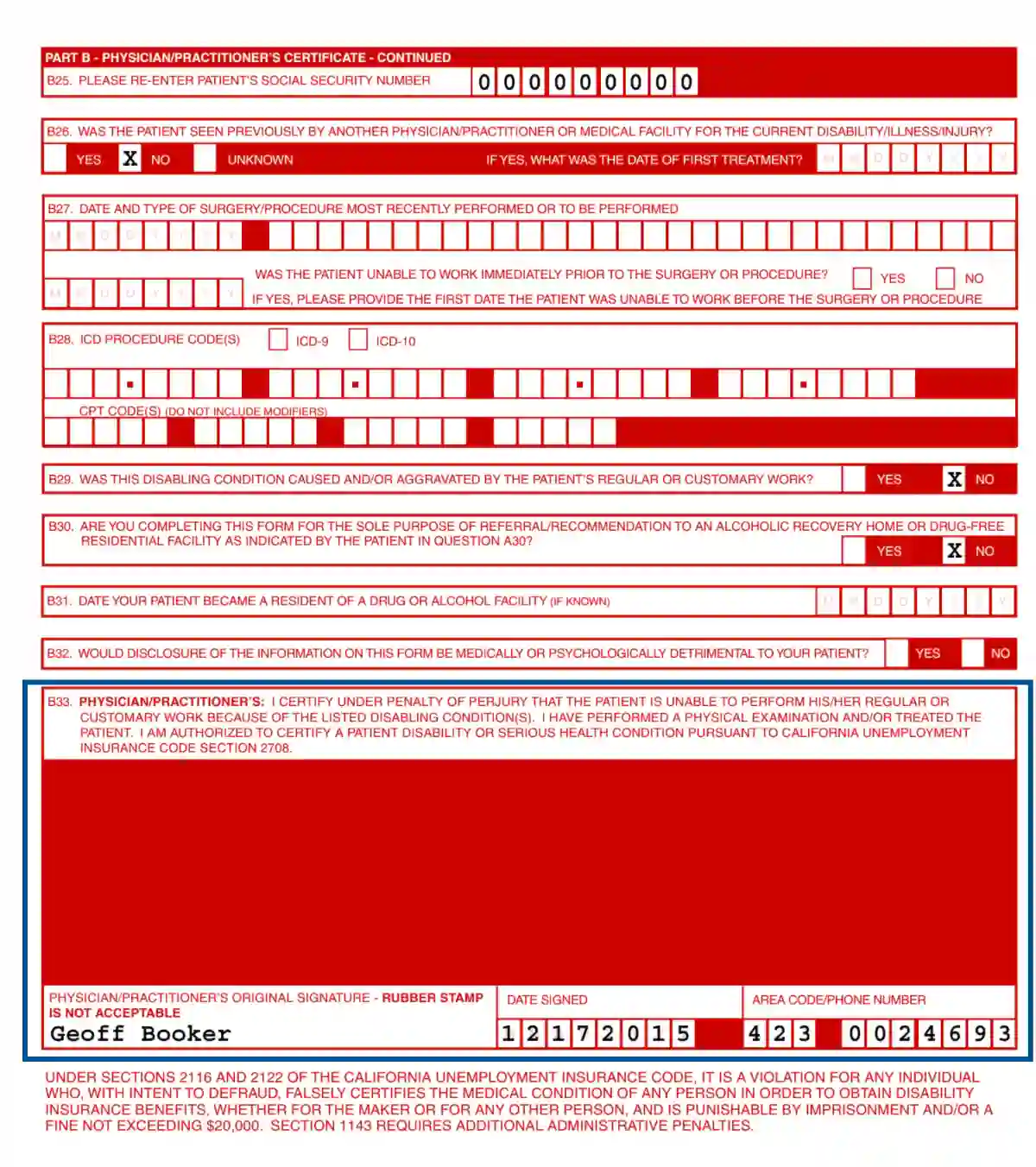
17. In boxes B25— B28, input the Social Security number of the patient, info of the previous appointments with physicians, recent surgery, and ICD procedures.
18. Check the boxes in B29— B32:
19. Certify the patient’s disability, put a sign and a date