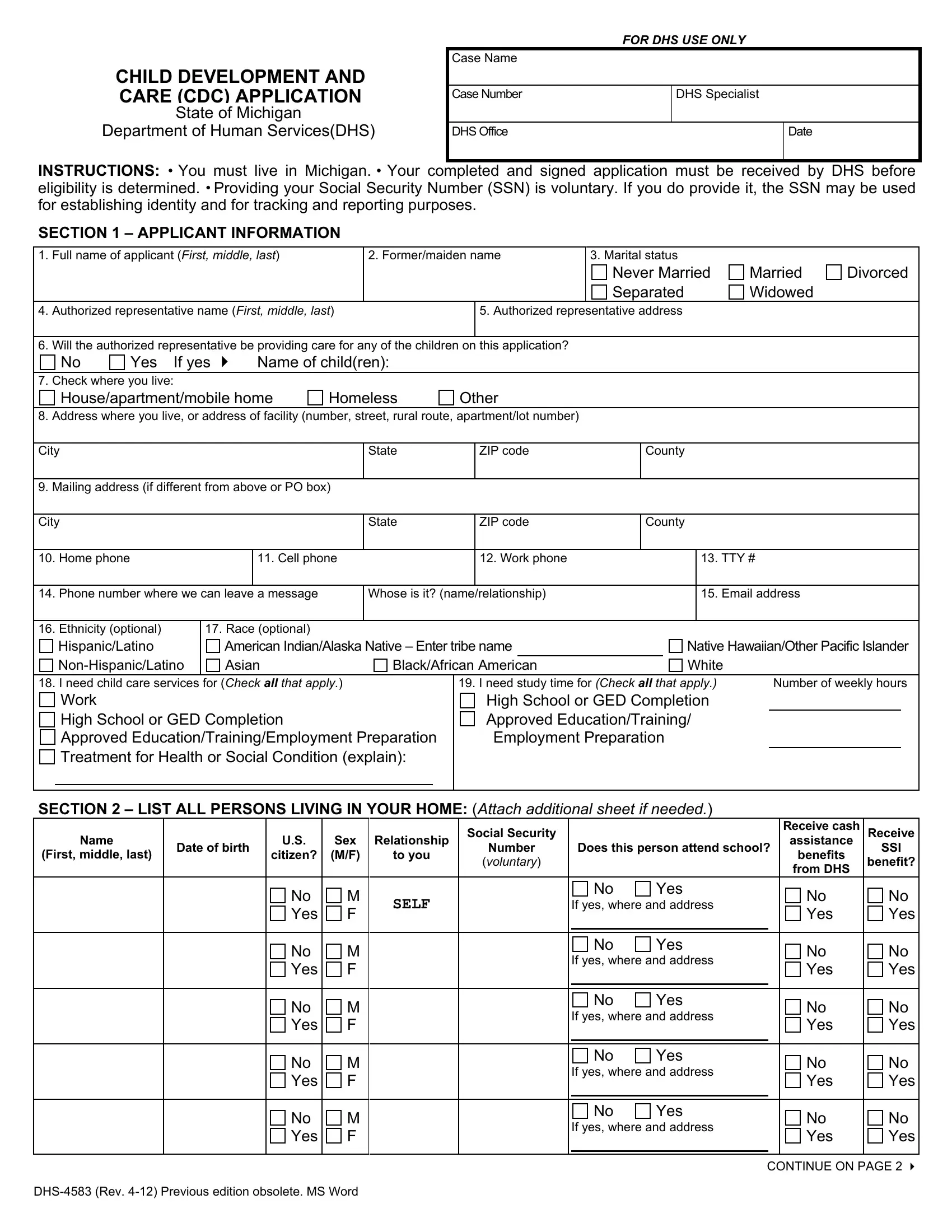
The DHS 4583 form, also known as the Child Development and Care (CDC) Application, plays a crucial role in the State of Michigan's efforts to support families in need of child care services. Managed by the Department of Human Services (DHS), this form serves as the initial step for caregivers living in Michigan to apply for child care assistance, ensuring that the state can determine their eligibility for such services. Applicants are instructed to provide comprehensive details about themselves, including residency status, Social Security Number (which is optional but aids in identity verification and tracking), and information pertaining to the children requiring care. The form not only captures basic demographics but also dives into the specifics of the child care needs based on the parents' work, study schedules, or involvement in health or social services. Additionally, the DHS 4583 form collects information on household composition, employment and income details, unearned income, and even offers an opportunity for voter registration, highlighting the thorough nature of the application process. Importantly, the instructions emphasize the necessity of honesty and timely reporting of any changes to avoid fraud charges or penalties, ensuring applicants are aware of their rights and responsibilities. This form is an essential document for Michigan residents seeking support for child care services, facilitating a better future for children and their families while maintaining compliance with state requirements.
| Question | Answer |
|---|---|
| Form Name | Dhs 4583 Form |
| Form Length | 5 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 1 min 15 sec |
| Other names | CDC, DHS-4583, Michigan, SSN |
