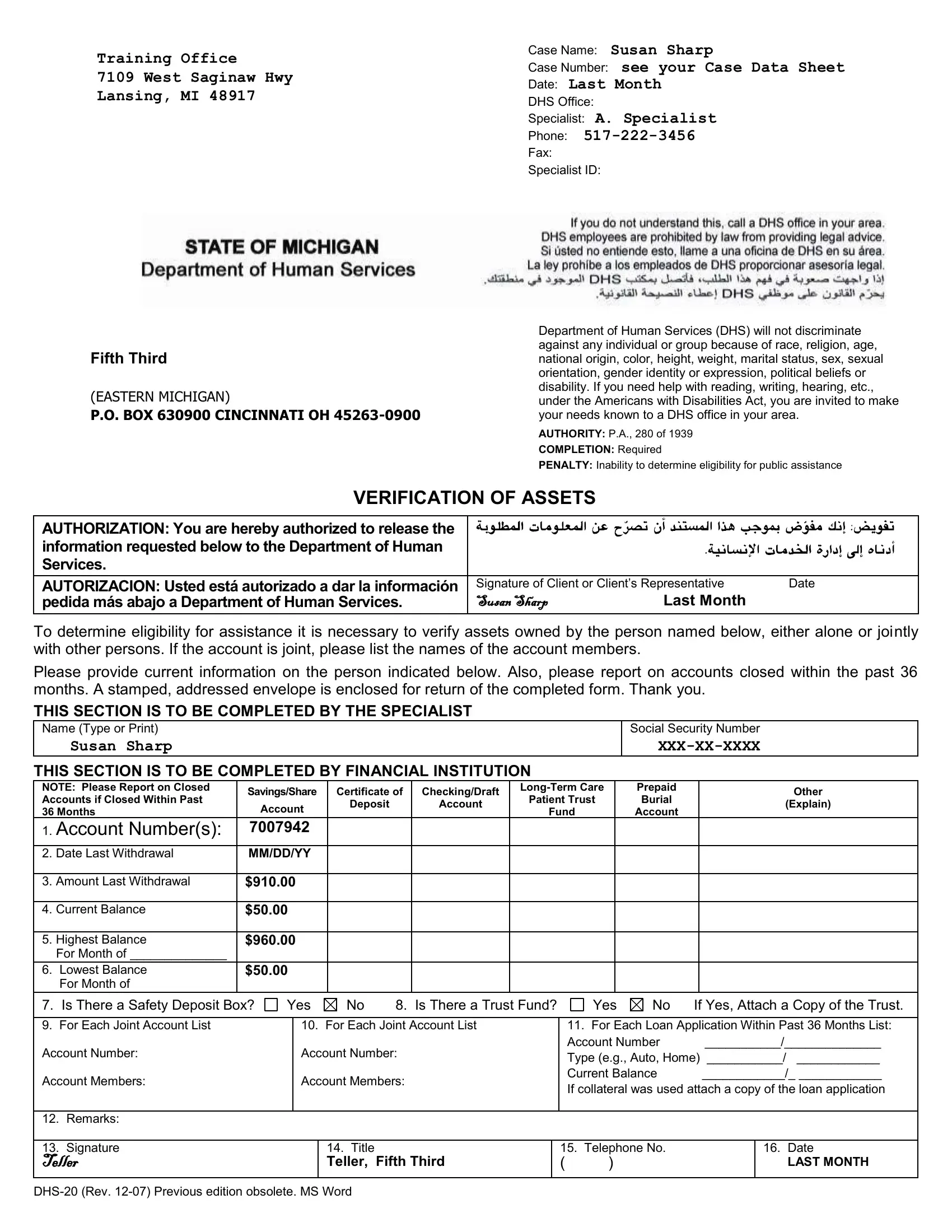
In the realm of navigating the intricacies of public assistance, the DHS 20 form stands as a vital document meant to streamline the process of verifying an individual's assets for eligibility determination. Operating under the authority of P.A., 280 of 1939, its completion is not merely a formality but a mandatory step in ensuring that those in need receive the support they merit, without discrimination. By authorizing the release of financial information, the form facilitates a crucial exchange between individuals—or their representatives—and financial institutions. This exchange is not limited to current asset statuses but extends to accounts closed within the past 36 months, ensuring a comprehensive view of one's financial history. The form pays deep respect to the diversity and needs of its constituents, clearly stating its adherence to the Americans with Disabilities Act by offering assistance to those who struggle with reading, writing, hearing, and more. This emblem of administrative diligence and inclusivity does more than merely gather data; it embodies the Department of Human Services' commitment to fairness and accessibility. With sections meticulously designed for both the applicant and the financial institution, it ensures clarity and completeness in the documentation of assets, from savings accounts to safety deposit boxes, all while upholding the privacy and dignity of all individuals.
| Question | Answer |
|---|---|
| Form Name | DHS-20 Form |
| Form Length | 1 pages |
| Fillable? | Yes |
| Fillable fields | 41 |
| Avg. time to fill out | 8 min 31 sec |
| Other names | dhs 20 verification of assets, michigan dhs 20 verification of assests form, dhs verification of assets form, dhs 20 |
