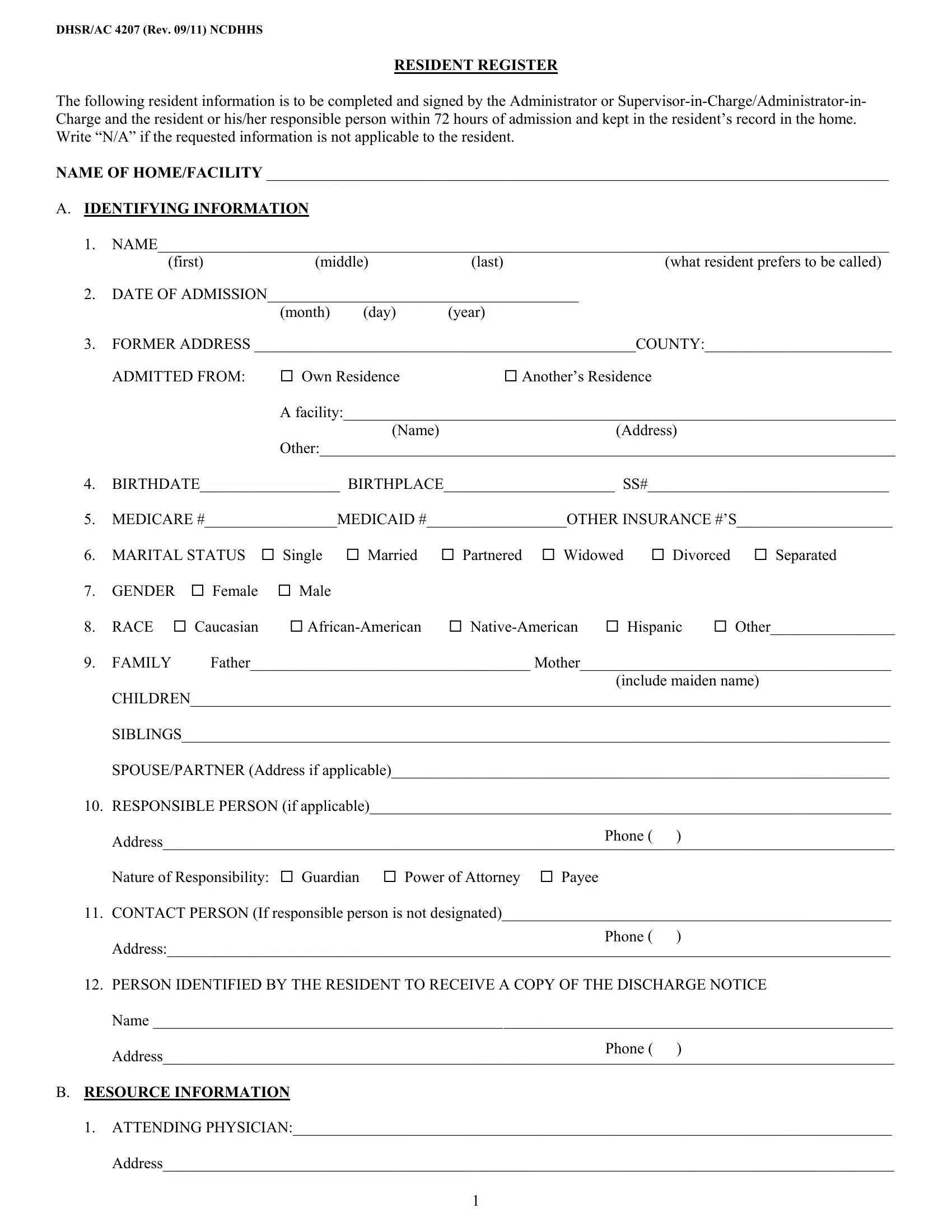
When individuals enter into a care facility, a document known as the DHSR/AC 4207 form becomes a crucial part of their admission process. This form, revised in September 2011 by the North Carolina Department of Health and Human Services (NCDHHS), serves as a comprehensive resident register, laying the groundwork for personalized and attentive care. Within 72 hours of admission, the form necessitates the gathering and recording of a wide array of personal information about the resident. It includes basic identifying details, such as name, date of admission, former address, social security number, medicare and medicaid numbers, marital status, gender, race, and contacts for family members and responsible persons. Moreover, the form covers a breadth of information regarding the resident’s health, including attending physician details, known allergies, food preferences, needed assistance, and personal habits. The DHSR/AC 4207 form also illustrates plans for payment of personal needs, community involvement interests, activities preferences, and the management of the resident’s personal funds and valuables. It necessitates signatures to validate the collation of information, acknowledgment of receipt of materials like the resident contract and home’s grievance procedures, and annual reviews or revisions of the information provided. Overall, this form plays a pivotal role in ensuring that residents receive a care plan tailored to their individual needs, rights, and preferences, fostering an environment of respect and dignity within the care facility.
| Question | Answer |
|---|---|
| Form Name | Dhsr Ac 4207 Form |
| Form Length | 4 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 1 min |
| Other names | dhsr ac register, form dhsr ac, dhsr 4207, dhsr 4207 ncdhhs |
