DIXIE STATE UNIVERSITY
Transcript Request Form
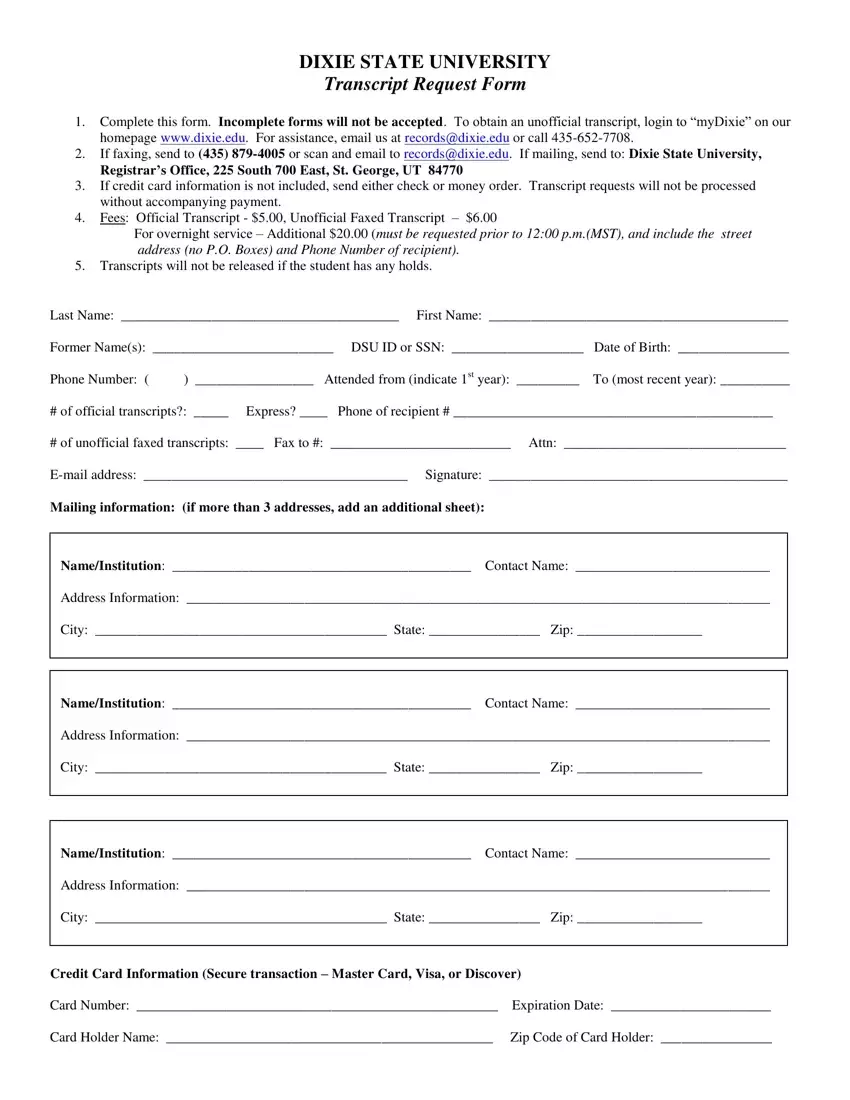
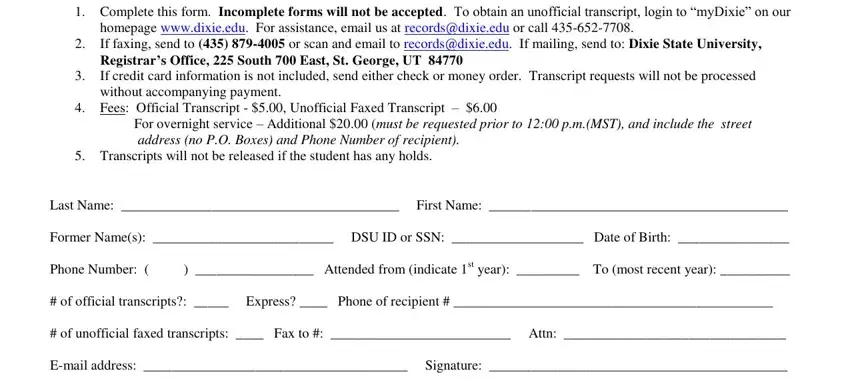
1.Complete this form. Incomplete forms will not be accepted. To obtain an unofficial transcript, login to “myDixie” on our homepage www.dixie.edu. For assistance, email us at records@dixie.edu or call 435-652-7708.
2.If faxing, send to (435) 879-4005 or scan and email to records@dixie.edu. If mailing, send to: Dixie State University,
Registrar’s Office, 225 South 700 East, St. George, UT 84770
3.If credit card information is not included, send either check or money order. Transcript requests will not be processed without accompanying payment.
4.Fees: Official Transcript - $5.00, Unofficial Faxed Transcript – $6.00
For overnight service – Additional $20.00 (must be requested prior to 12:00 p.m.(MST), and include the street address (no P.O. Boxes) and Phone Number of recipient).
5.Transcripts will not be released if the student has any holds.
Last Name: ________________________________________ First Name: ___________________________________________
|
|
|
|
Former Name(s): __________________________ |
DSU ID or SSN: ___________________ |
Date of Birth: ________________ |
Phone Number: ( |
) _________________ Attended from (indicate 1st year): _________ |
To (most recent year): __________ |
# of official transcripts?: _____ Express? ____ |
Phone of recipient # ______________________________________________ |
# of unofficial faxed transcripts: ____ Fax to #: __________________________ Attn: ________________________________
E-mail address: ______________________________________ Signature: ___________________________________________
Mailing information: (if more than 3 addresses, add an additional sheet):
Name/Institution: ___________________________________________ Contact Name: ____________________________
Address Information: ____________________________________________________________________________________
City: __________________________________________ State: ________________ Zip: __________________
Name/Institution: ___________________________________________ Contact Name: ____________________________
Address Information: ____________________________________________________________________________________
City: __________________________________________ State: ________________ Zip: __________________
Name/Institution: ___________________________________________ Contact Name: ____________________________
Address Information: ____________________________________________________________________________________
City: __________________________________________ State: ________________ Zip: __________________
Credit Card Information (Secure transaction – Master Card, Visa, or Discover)
Card Number: ____________________________________________________ |
Expiration Date: _______________________ |
Card Holder Name: _______________________________________________ |
Zip Code of Card Holder: ________________ |