Our best developers have worked together to implement the PDF editor which you will take advantage of. The software enables you to get fillable dmas 225 documentation instantly and without problems. This is certainly all you should conduct.
Step 1: The first thing is to select the orange "Get Form Now" button.
Step 2: You're now ready to update fillable dmas 225. You've got a wide range of options thanks to our multifunctional toolbar - you can include, remove, or change the information, highlight the specific sections, and perform many other commands.
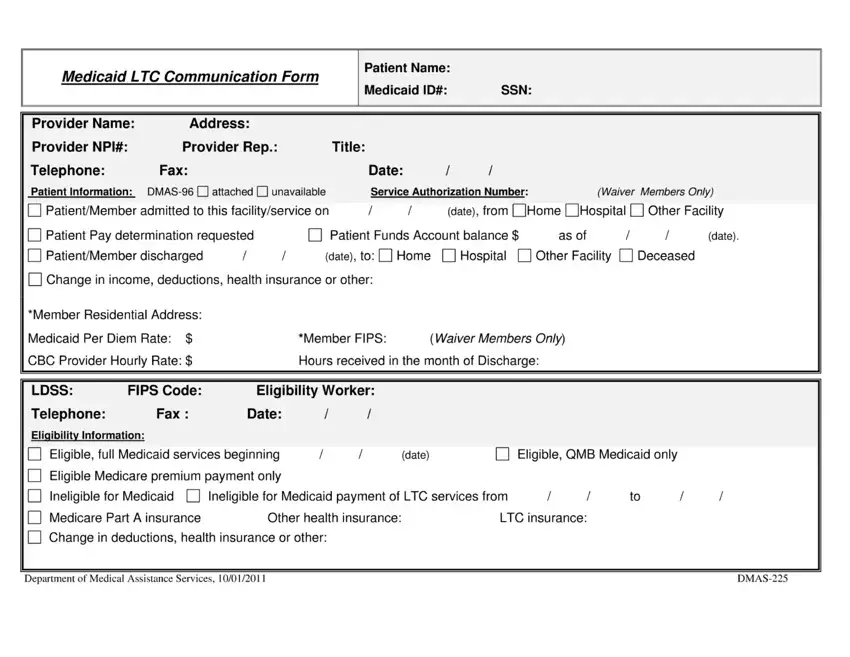
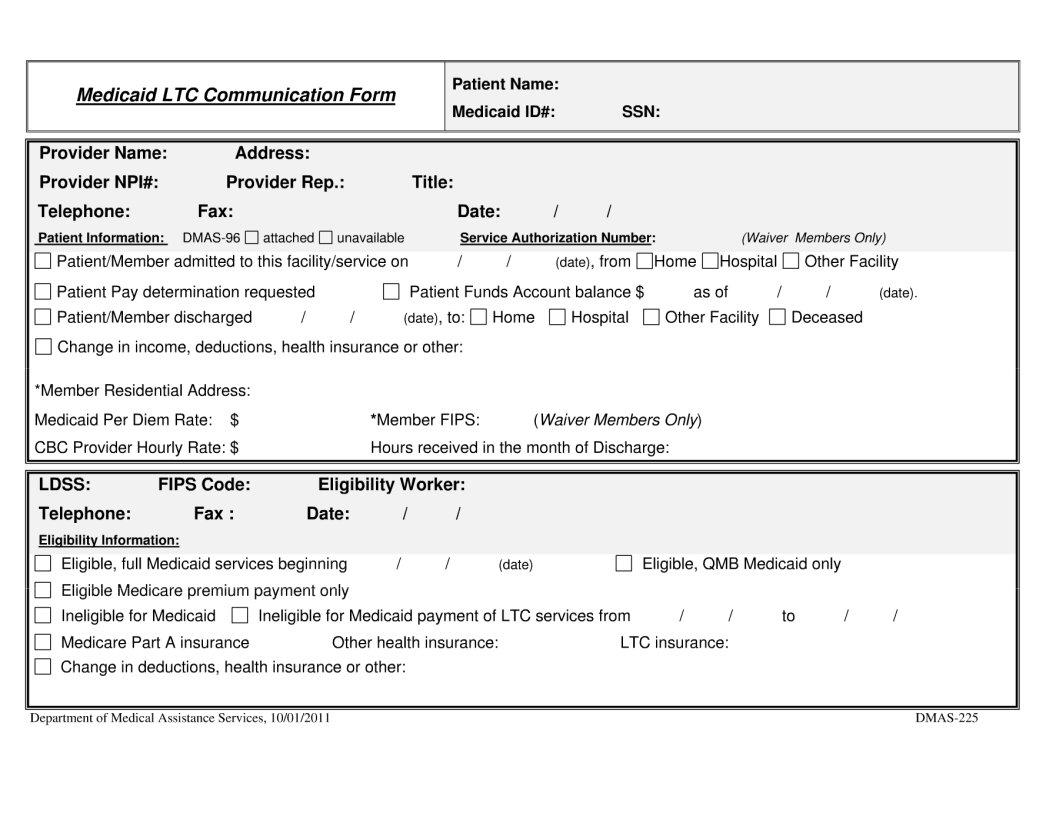
To fill out the file, type in the content the program will require you to for each of the appropriate parts:
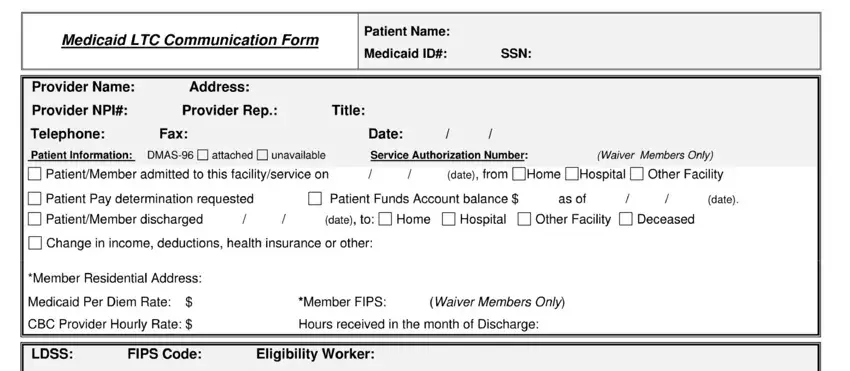
The program will require you to complete the LDS, S, Telephone, Eligibility, Information Eligible, QM, B, Medicaid, only Other, health, insurance LT, C, insurance date, and DM, AS field.
Step 3: Choose the Done button to be certain that your completed file is available to be transferred to any kind of gadget you prefer or sent to an email you specify.
Step 4: In order to avoid potential future problems, ensure that you hold minimally a pair of duplicates of each separate document.
