

Handling PDF files online is certainly quite easy using our PDF tool. You can fill out medicare intake here and try out many other functions we offer. To have our editor on the leading edge of practicality, we strive to adopt user-oriented capabilities and improvements on a regular basis. We're always pleased to get suggestions - join us in reshaping PDF editing. Getting underway is simple! All you have to do is adhere to these basic steps directly below:
Step 1: First of all, open the editor by clicking the "Get Form Button" above on this webpage.
Step 2: With the help of our state-of-the-art PDF file editor, you're able to do more than merely fill in blank fields. Try all the functions and make your forms seem great with customized text added, or modify the file's original input to perfection - all backed up by the capability to add stunning photos and sign the document off.
Concentrate while filling out this document. Ensure each and every blank is filled out correctly.
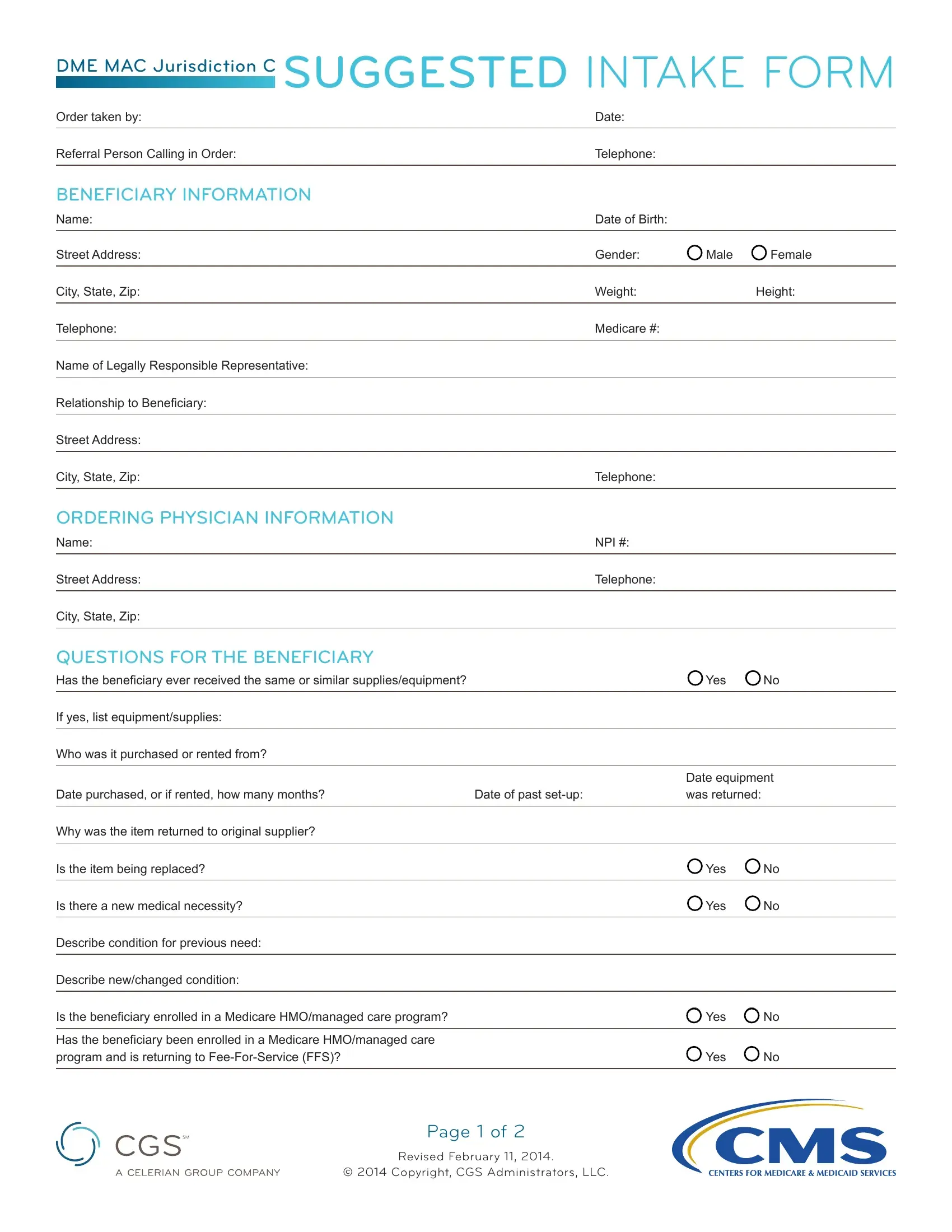
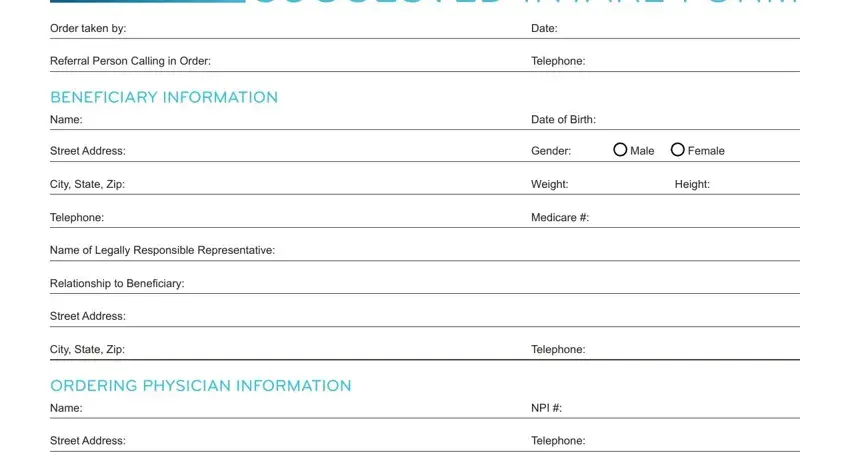
1. For starters, while filling out the medicare intake, start out with the form section that contains the following blank fields:
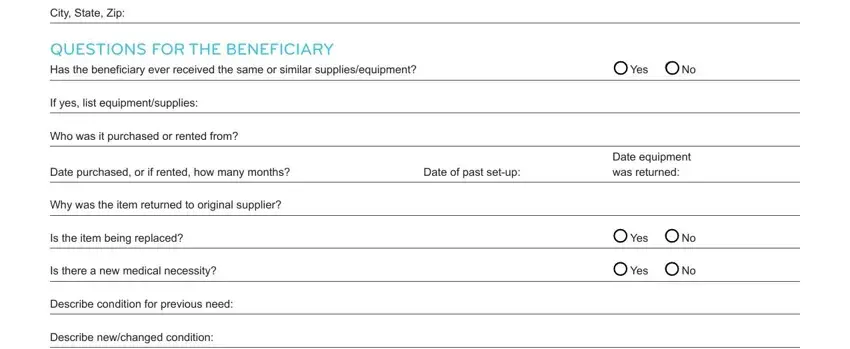
2. The subsequent part is to complete the next few blank fields: City State Zip, QUESTIONS FOR THE BENEFICIARY, Has the beneficiary ever received, If yes list equipmentsupplies, Who was it purchased or rented from, Date purchased or if rented how, Date of past setup, Why was the item returned to, Is the item being replaced, Is there a new medical necessity, Describe condition for previous, Describe newchanged condition, Yes No, Date equipment was returned, and Yes No.
3. Within this step, look at Is the beneficiary enrolled in a, Has the beneficiary been enrolled, Yes No, Yes No, Page of, Revised February, and Copyright CGS Administrators LLC. Each of these are required to be completed with utmost attention to detail.
4. This particular paragraph arrives with these blanks to fill out: QUESTIONS FOR THE SUPPLIER If, Manufacturer, Model Name or, Serial, Purchase Date, Reason or nature of repairs, Do you have medical necessity to, Does beneficiary meet criteria for, Questions for the Supplier, Where will the item be used, SIGNATURE, Beneficiary Signature, Yes No, Yes No, and Date Signed.
In terms of Do you have medical necessity to and Purchase Date, make sure that you do everything right here. Both of these are definitely the key ones in the file.
Step 3: Just after proofreading the fields and details, hit "Done" and you are done and dusted! Get hold of your medicare intake as soon as you register at FormsPal for a 7-day free trial. Easily use the pdf file inside your FormsPal account, together with any edits and adjustments being conveniently synced! We don't share any details you type in while dealing with documents at our website.