
handicap placard virginia can be filled in online with ease. Just try FormsPal PDF editor to finish the job without delay. Our editor is continually developing to deliver the best user experience possible, and that is thanks to our dedication to constant enhancement and listening closely to customer comments. In case you are looking to begin, this is what it's going to take:
Step 1: Access the PDF file inside our tool by pressing the "Get Form Button" at the top of this page.
Step 2: The editor will give you the opportunity to modify your PDF document in various ways. Enhance it by writing personalized text, correct original content, and include a signature - all when it's needed!
If you want to finalize this PDF form, make sure that you type in the information you need in each field:
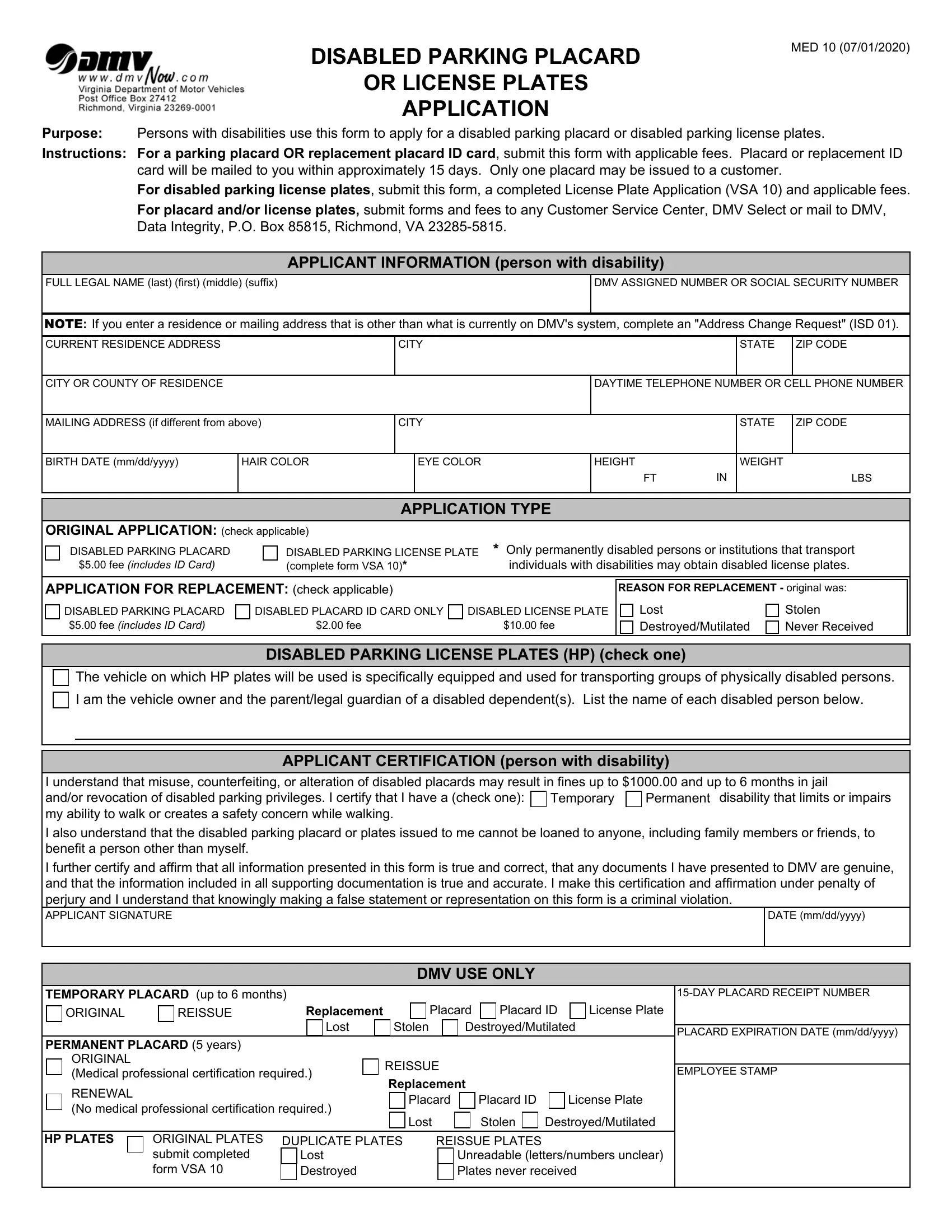
1. Fill out your handicap placard virginia with a group of essential fields. Collect all the important information and be sure not a single thing omitted!
2. Soon after filling out this part, go to the next step and enter all required details in all these blanks - I am the vehicle owner and the, APPLICANT CERTIFICATION person, I understand that misuse, DATE mmddyyyy, Temporary, Permanent, TEMPORARY PLACARD up to months, DAY PLACARD RECEIPT NUMBER, ORIGINAL, REISSUE, Replacement, Placard, Placard ID, License Plate, and Lost.
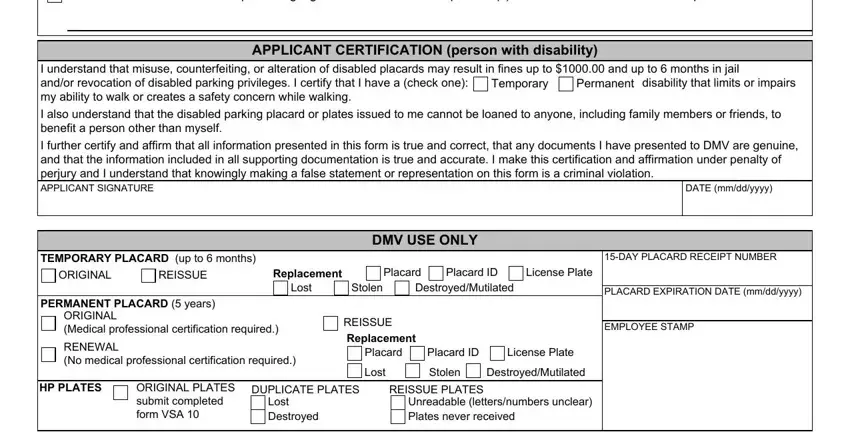
You can easily make a mistake while completing your DATE mmddyyyy, for that reason make sure to reread it prior to when you send it in.
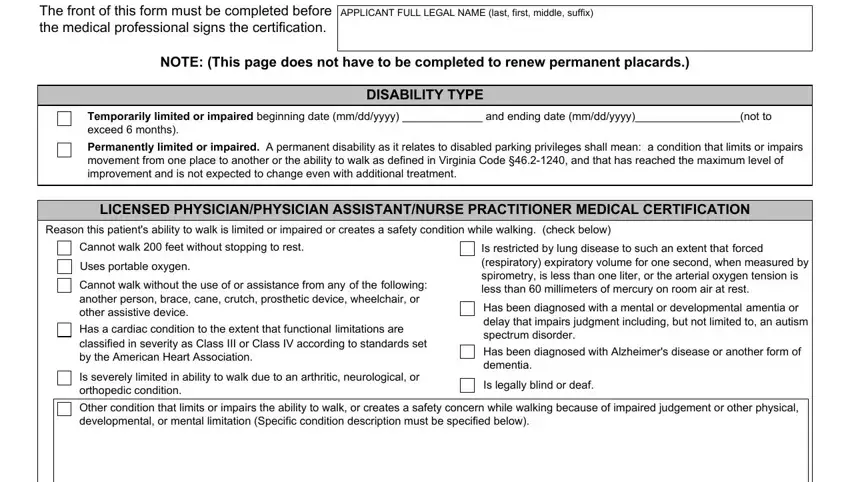
3. Within this stage, look at The front of this form must be, APPLICANT FULL LEGAL NAME last, NOTE This page does not have to be, DISABILITY TYPE, Temporarily limited or impaired, Permanently limited or impaired A, LICENSED PHYSICIANPHYSICIAN, Reason this patients ability to, Cannot walk feet without stopping, Uses portable oxygen Cannot walk, Is restricted by lung disease to, Is severely limited in ability to, Is legally blind or deaf, and Other condition that limits or. Each of these need to be filled out with highest precision.
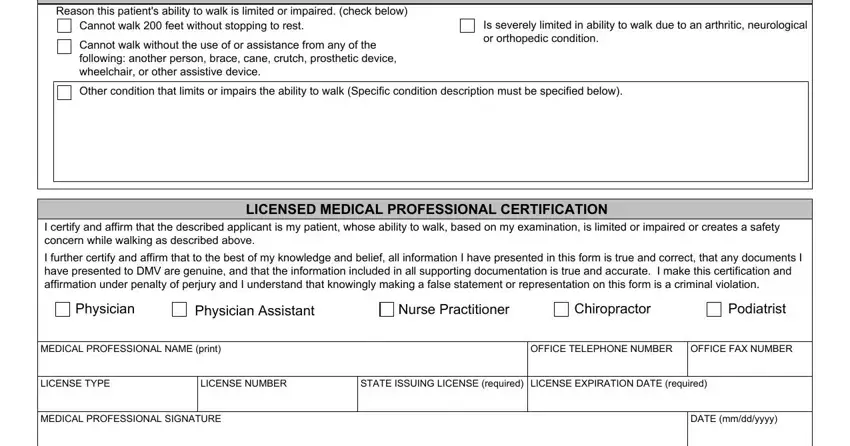
4. This specific part comes next with the next few form blanks to fill out: LICENSED CHIROPRACTOR OR, Reason this patients ability to, Cannot walk feet without stopping, Cannot walk without the use of or, Is severely limited in ability to, Other condition that limits or, LICENSED MEDICAL PROFESSIONAL, I certify and affirm that the, I further certify and affirm that, Physician, Physician Assistant, Nurse Practitioner, Chiropractor, Podiatrist, and MEDICAL PROFESSIONAL NAME print.
Step 3: Confirm that the information is right and then press "Done" to proceed further. Acquire the handicap placard virginia as soon as you join for a 7-day free trial. Easily access the pdf from your personal cabinet, along with any edits and changes conveniently kept! FormsPal is focused on the personal privacy of our users; we always make sure that all information used in our system continues to be protected.