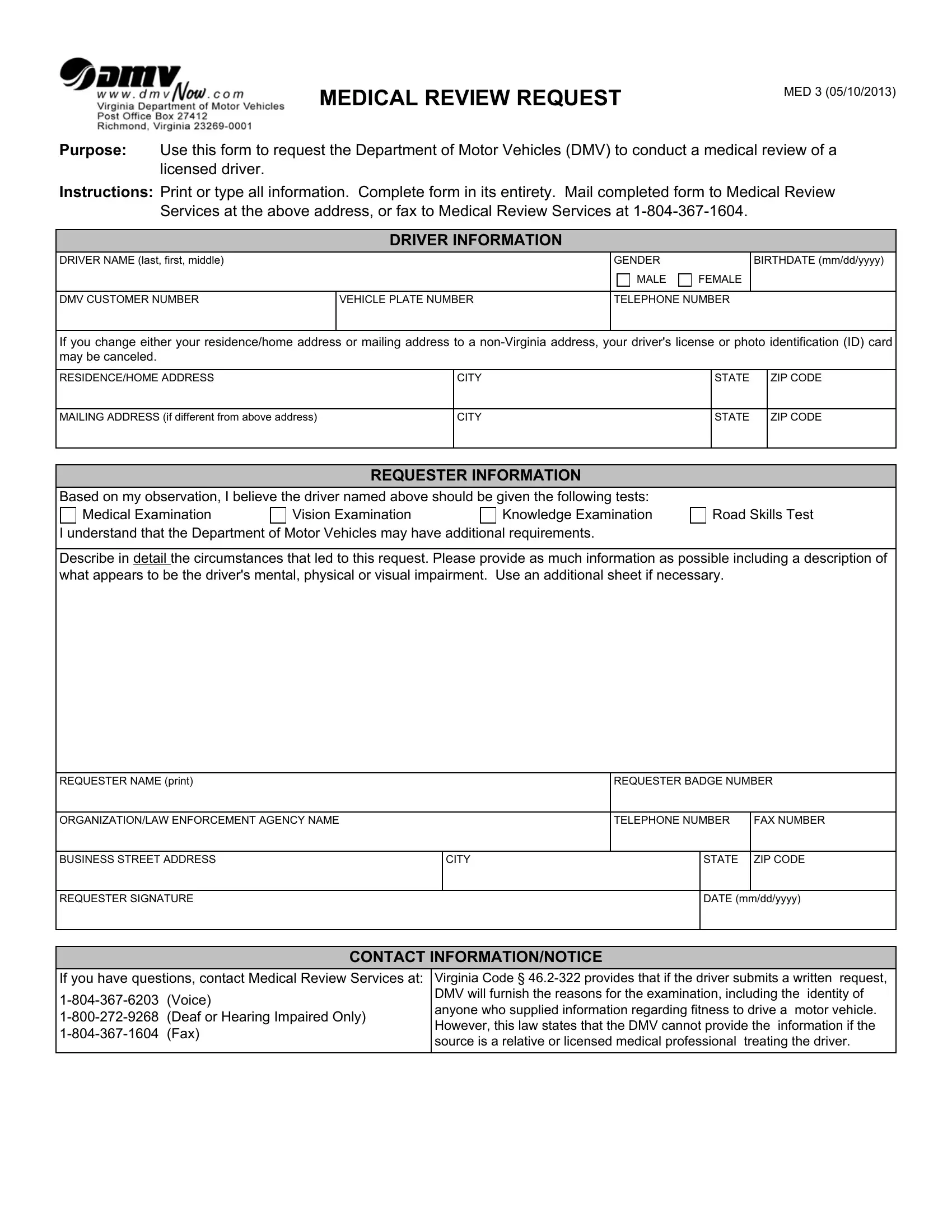
The DMV Med 3 form is a crucial document designed for those who see the need to request a medical review for a licensed driver, possibly due to concerns over their ability to safely operate a vehicle. This comprehensive form aims to facilitate this process by gathering detailed information about the driver in question, including their personal details and any observations related to their mental, physical, or visual capabilities that may affect their driving abilities. The form not only allows the requestor to specify the type of examinations (medical, vision, knowledge, and road skills test) they believe should be conducted but also provides space for an in-depth description of the circumstances and behaviors observed that led to the concern. To complete the MED 3, one must provide both the driver's and the requester's information, ensuring the DMV can follow up effectively. This includes names, addresses, and contact details, alongside the requester's association and signature to officially lodge the request. Once filled, the form can be mailed or faxed to the Medical Review Services, demonstrating the DMV's commitment to road safety by examining drivers whose capabilities may be in question. It's important for requestors to note that the involved driver can request the reasons for the examination, highlighting a transparent process, albeit with anonymity protected for certain informants like relatives or the driver's medical professionals.
| Question | Answer |
|---|---|
| Form Name | Dmv Form Med 3 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | mailing, Impaired, impairment, furnish |
