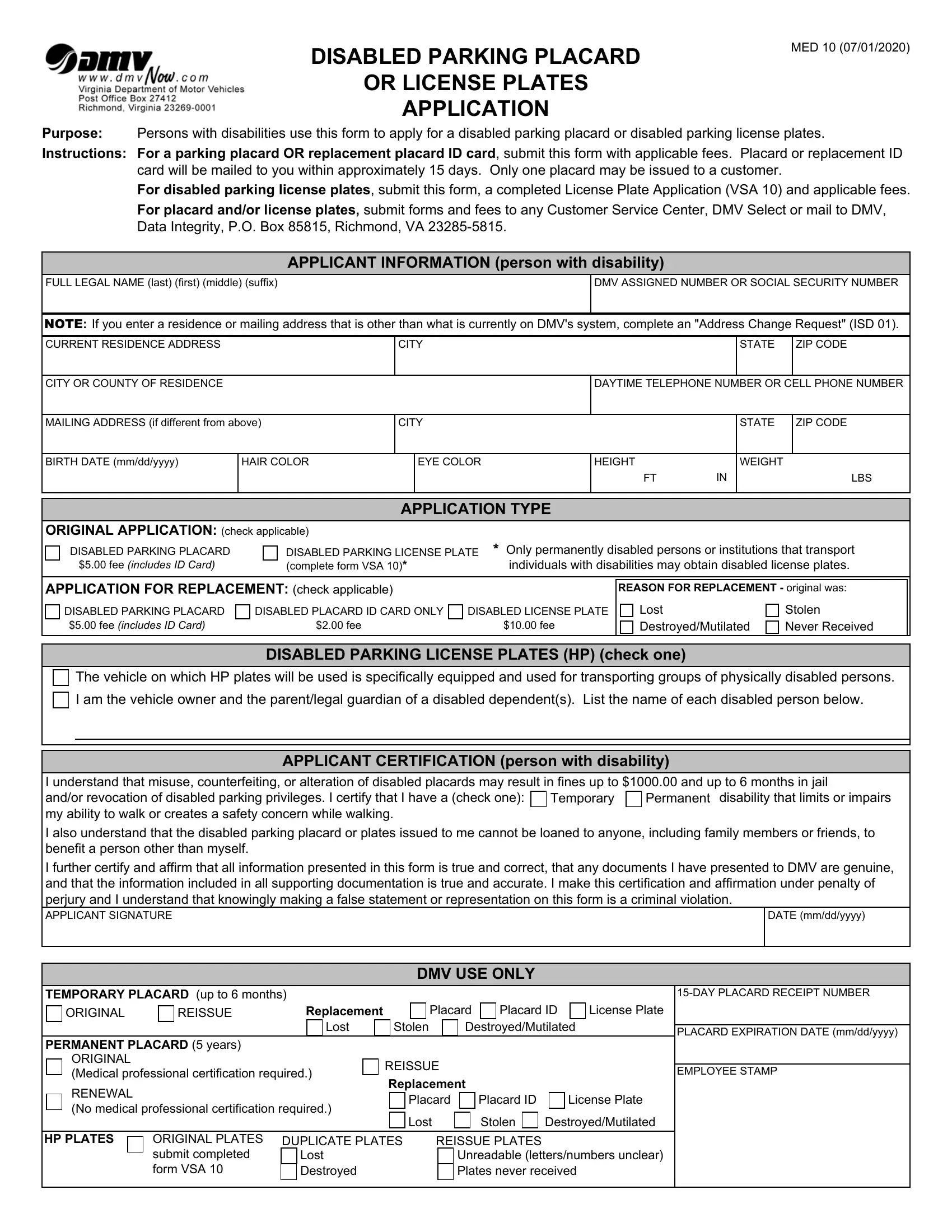
Providing accessible parking options to individuals with disabilities is a fundamental aspect of fostering inclusivity and accessibility in public spaces. The DMV Med 10 form serves as a critical tool in this endeavor, enabling persons with disabilities to apply for disabled parking placards or license plates. Taking effect from July 1, 2020, this form not only standardizes the application process but also specifies the conditions under which eligibility is determined and the types of parking aids available. Applicants are required to furnish detailed personal information, undergo a certification process by a licensed medical professional, and choose between a placard or license plate, depending on their needs or the nature of their disability. Importantly, the form highlights that the misuse of issued placards or plates, including lending them to others, may result in significant penalties, underscoring the legal and ethical responsibilities that come with the issuance of such parking aids. To streamline the process, the form outlines how to apply for replacements in case of loss, theft, or damage and delineates the fees associated with each application type. By providing a structured way to apply for and renew disabled parking permits, the DMV Med 10 form plays a pivotal role in ensuring equal access and convenience for individuals with disabilities, thus contributing to their autonomy and mobility.
| Question | Answer |
|---|---|
| Form Name | Dmv Form Med 10 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | virginia disabled parking, dmv handicap form, dmv disability form, disabled parking placard application |