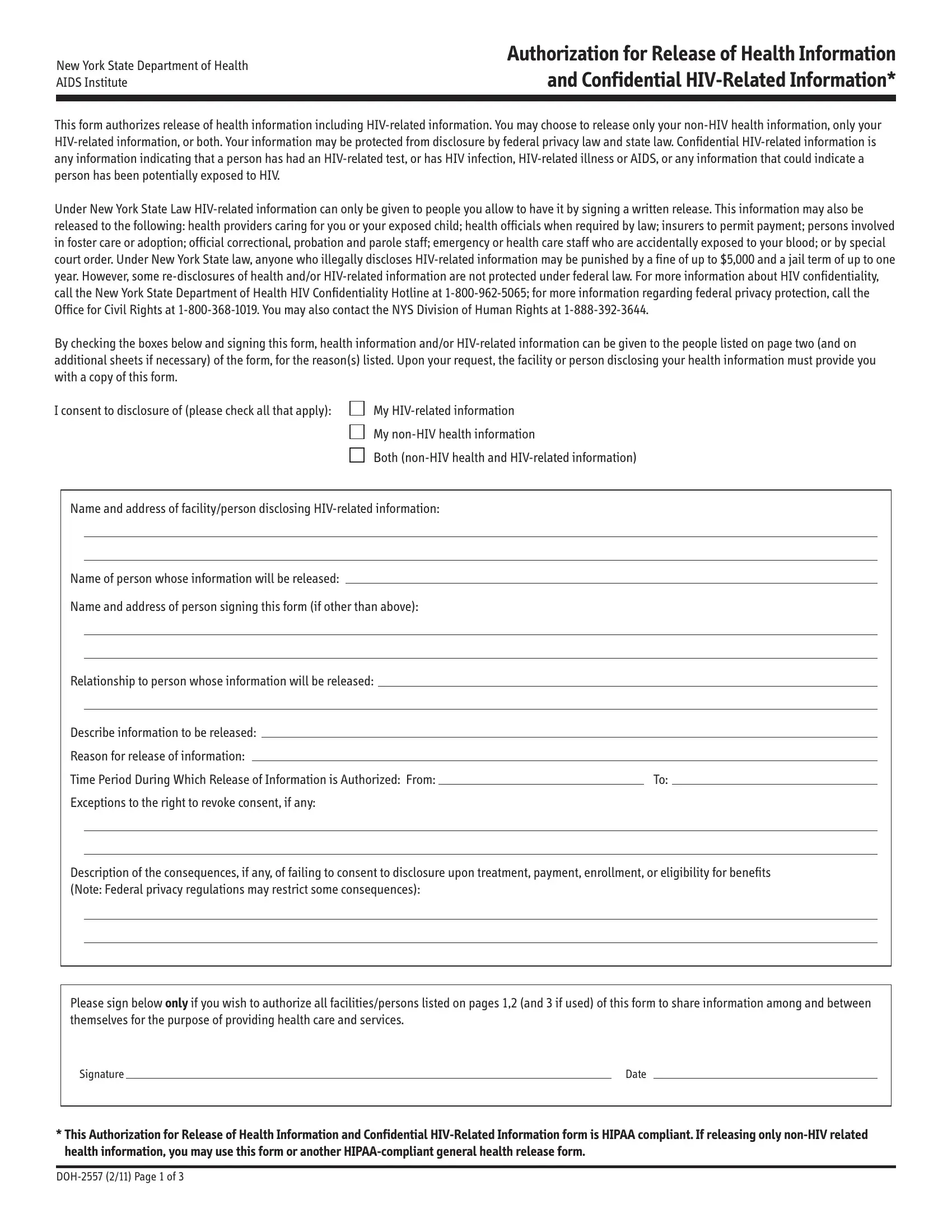
When individuals need to manage the release of their sensitive health information, especially when it pertains to HIV-related details, the New York State Department of Health AIDS Institute offers a crucial document: the DOH 2557 form. This document is not just another form; it is a gateway to ensuring privacy, complying with both federal privacy laws and New York State law, and controlling who has access to one’s personal health information. Whether an individual chooses to release all or only specific parts of their health information, this form stands as their written consent to do so, safeguarding their rights and determining the flow of their confidential information to designated parties. By selecting to release either all, none, or some of their HIV-related information, individuals assert their autonomy over personal health details in circumstances ranging from healthcare provision to legal and correctional situations. Importantly, the form outlines the potential consequences of unauthorized disclosure, emphasizing the protected nature of this information under law, and outlines the fines and penalties for breaches of confidentiality. Furthermore, it ensures that any release of information aligns with HIPAA (Health Insurance Portability and Accountability Act), reinforcing the safeguarding of patient privacy in a healthcare context. This form also serves as a reminder of the individual’s rights, including the right to retract consent at any time, showcasing the balance between necessary information sharing and the maintenance of personal privacy and dignity.
| Question | Answer |
|---|---|
| Form Name | Doh 2557 Form |
| Form Length | 3 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 45 sec |
| Other names | information confidential related, releasing doh, form hipaa doh form, form 2557 |
New York State Department of Health AIDS Institute
Authorization for Release of Health Information and Confidential
This form authorizes release of health information including
Under New York State Law
By checking the boxes below and signing this form, health information and/or
I consent to disclosure of (please check all that apply):
My
My
Both
Name and address of facility/person disclosing
Name of person whose information will be released:
Name and address of person signing this form (if other than above):
Relationship to person whose information will be released:
Describe information to be released:
Reason for release of information:
Time Period During Which Release of Information is Authorized: From: |
|
To: |
|
|
Exceptions to the right to revoke consent, if any: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Description of the consequences, if any, of failing to consent to disclosure upon treatment, payment, enrollment, or eligibility for benefits (Note: Federal privacy regulations may restrict some consequences):
Please sign below only if you wish to authorize all facilities/persons listed on pages 1,2 (and 3 if used) of this form to share information among and between themselves for the purpose of providing health care and services.
Signature |
|
Date |
*This Authorization for Release of Health Information and Confidential
Authorization for Release of Health Information and Confidential
Complete information for each facility/person to be given general information and/or
Name and address of facility/person to be given general health and/or
Reason for release, if other than stated on page 1:
If information to be disclosed to this facility/person is limited, please specify:
Name and address of facility/person to be given general health and/or
Reason for release, if other than stated on page 1:
If information to be disclosed to this facility/person is limited, please specify:
The law protects you from
My questions about this form have been answered. I know that I do not have to allow release of my health and/or
Signature |
|
|
Date |
|
(SUBJECT OF INFORMATION OR LEGALLY AUTHORIZED REPRESENTATIVE) |
||
If legal representative, indicate relationship to subject:
Print Name
Client/Patient Number
*This Authorization for Release of Health Information and Confidential
Authorization for Release of Health Information and Confidential
Complete information for each facility/person to be given general information and/or
Name and address of facility/person to be given general health and/or
Reason for release, if other than stated on page 1:
If information to be disclosed to this facility/person is limited, please specify:
Name and address of facility/person to be given general health and/or
Reason for release, if other than stated on page 1:
If information to be disclosed to this facility/person is limited, please specify:
Name and address of facility/person to be given general health and/or
Reason for release, if other than stated on page 1:
If information to be disclosed to this facility/person is limited, please specify:
If any/all of this page is completed, please sign below: |
|
|
|
||
Signature |
|
Date |
|
|
|
|
(SUBJECT OF INFORMATION OR LEGALLY AUTHORIZED REPRESENTATIVE) |
|
|
|
|
Client/Patient Number |
|
|
|
|
|
|
|
|
|
|
|
*This Authorization for Release of Health Information and Confidential