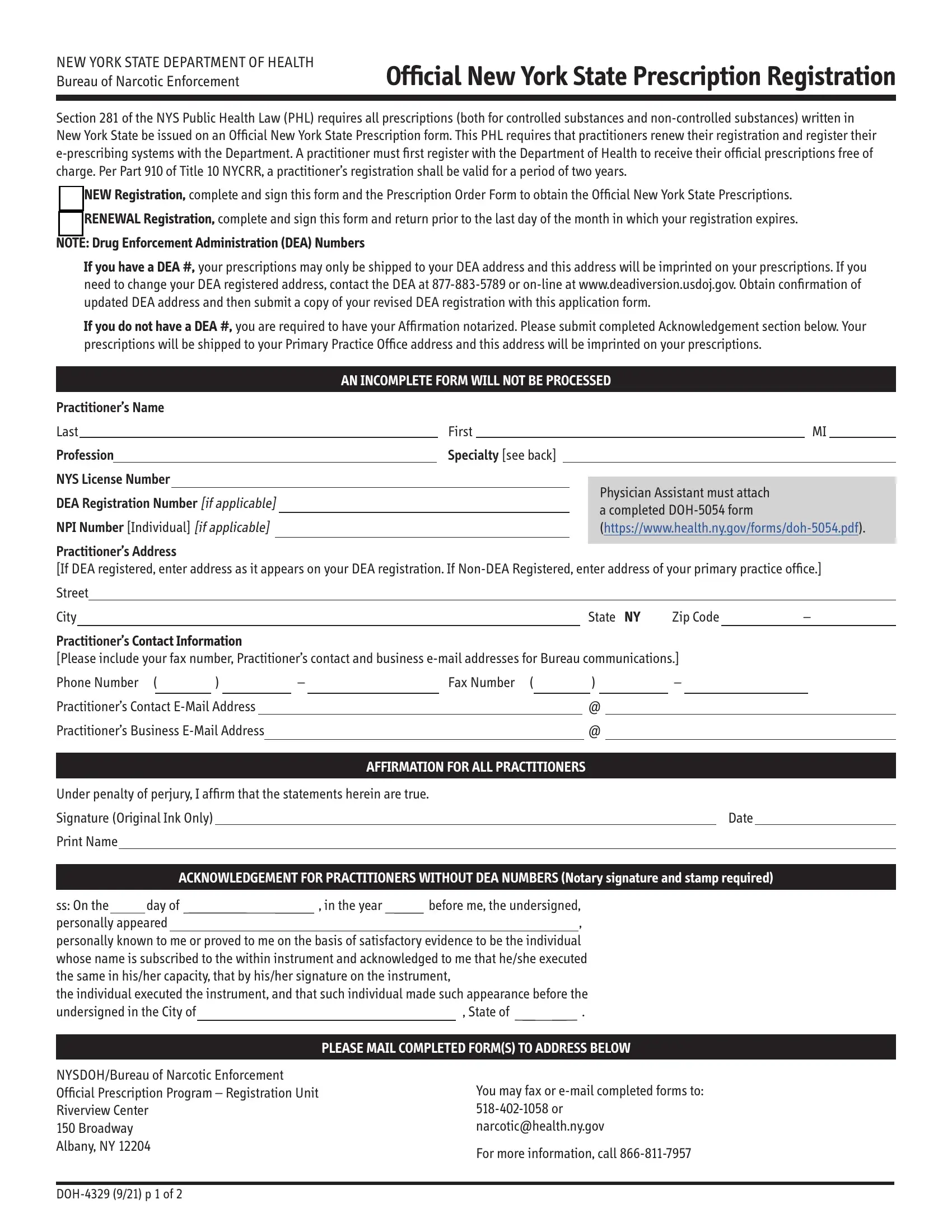
In New York State, the regulation of prescriptions is enhanced by the requirement that all such documents, whether for controlled or non-controlled substances, be issued on an Official New York State Prescription form, as underscored by Section 281 of the NYS Public Health Law (PHL). The DOH 4329 form plays a central role in this process, providing a means for practitioners to register or renew their registration with the Department of Health, thereby enabling them to issue official prescriptions. The Bureau of Narcotic Enforcement oversees this registration, which is valid for two years and mandates not only the completion of the DOH 4329 form but also the registration of e-prescribing systems. A noteworthy requirement for practitioners with a DEA number is that prescriptions can only be dispatched to the address registered with the DEA, underscoring the tight integration between state and federal regulatory frameworks. Moreover, for those without a DEA number, an affirmation needs to be notarized to complete the registration process. This setup ensures that every practitioner issuing prescriptions in New York adheres to a standardized protocol, ultimately aiming to enhance patient safety and regulatory compliance.
| Question | Answer |
|---|---|
| Form Name | DOH 4329 Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | Electronic Prescribing - New York State Department of Health - NY.gov |