


Should you wish to fill out new york state c4 forms, you won't need to download and install any applications - simply try using our PDF tool. In order to make our editor better and more convenient to work with, we continuously implement new features, considering feedback coming from our users. Starting is effortless! Everything you should do is stick to the following basic steps down below:
Step 1: Open the PDF doc inside our tool by pressing the "Get Form Button" in the top section of this webpage.
Step 2: This editor enables you to change your PDF in a variety of ways. Modify it with your own text, adjust what's already in the document, and put in a signature - all readily available!
This PDF form will require particular details to be typed in, therefore ensure that you take whatever time to fill in exactly what is expected:
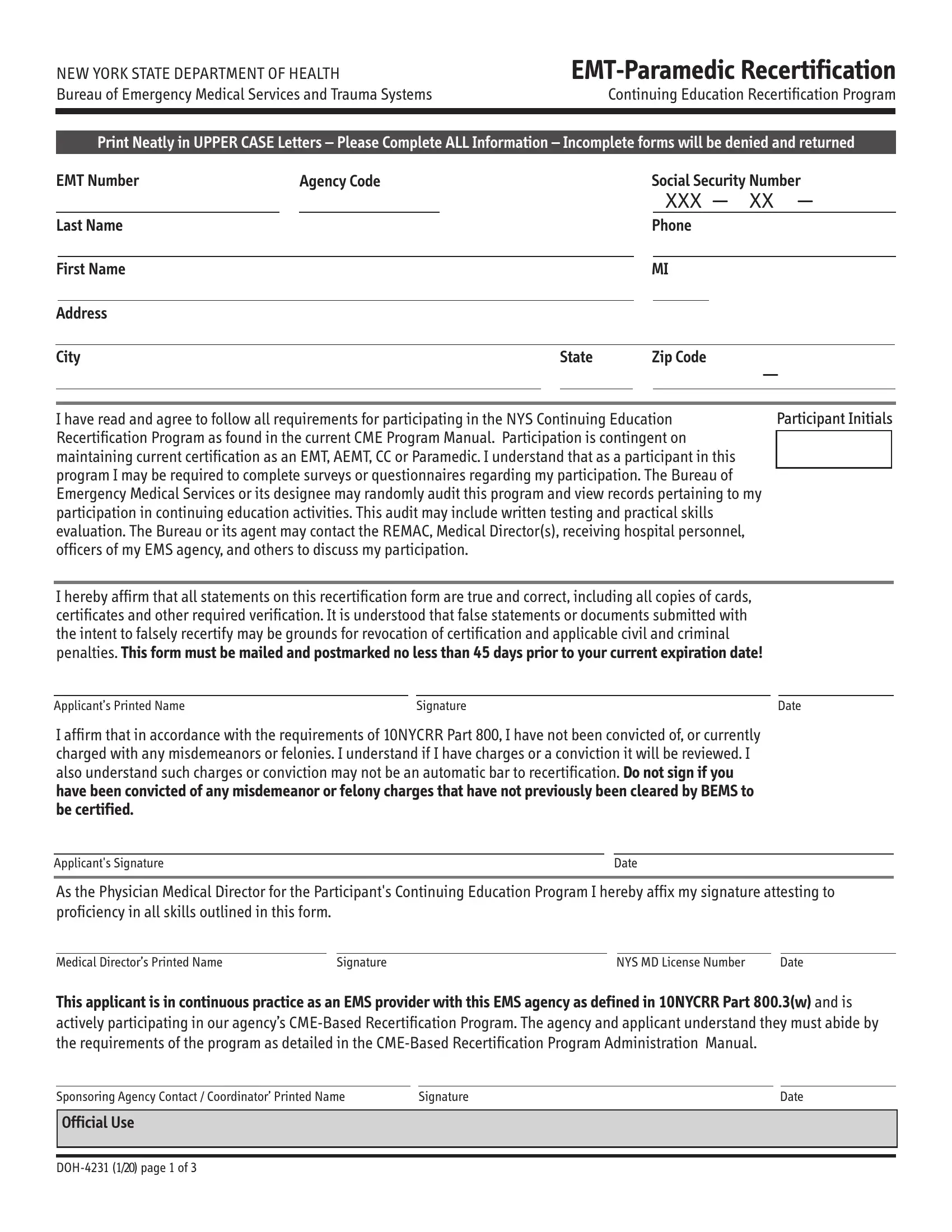
1. Before anything else, once completing the new york state c4 forms, start out with the area that contains the following blanks:
2. The next step is to fill out these particular fields: I hereby affirm that all, Applicants Printed Name, Signature, Date, I affirm that in accordance with, Applicants Signature, Date, As the Physician Medical Director, Medical Directors Printed Name, Signature, NYS MD License Number, Date, and This applicant is in continuous.
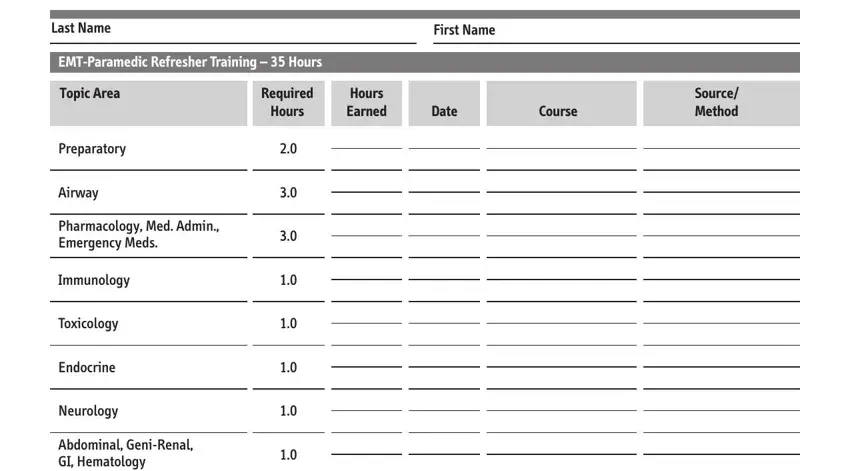
3. Completing Last Name, First Name, EMTParamedic Refresher Training, Topic Area, Preparatory, Airway, Pharmacology Med Admin Emergency, Immunology, Toxicology, Endocrine, Neurology, Abdominal GeniRenal GI Hematology, Required, Hours, and Hours Earned is essential for the next step, make sure to fill them out in their entirety. Don't miss any details!
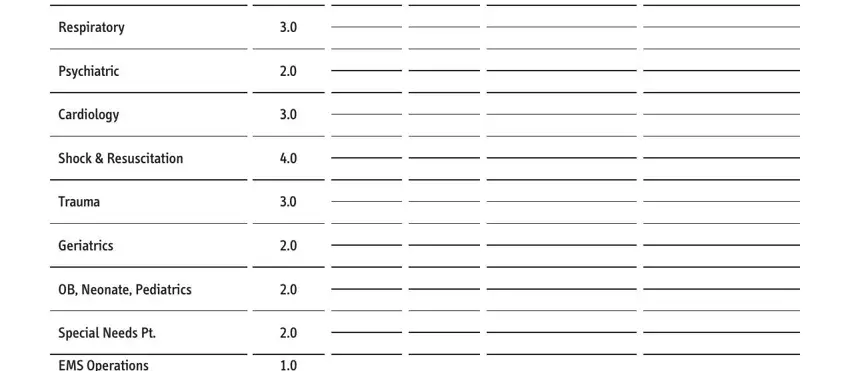
4. It's time to start working on this next part! In this case you'll have these Respiratory, Psychiatric, Cardiology, Shock Resuscitation, Trauma, Geriatrics, OB Neonate Pediatrics, Special Needs Pt, and EMS Operations fields to complete.
5. The last step to submit this PDF form is integral. You'll want to fill out the required fields, for instance EMS Operations, TOTALS, CIC Signature, CIC Print Name, CIC Number, and DOH page of, prior to finalizing. Neglecting to accomplish that can give you an unfinished and possibly nonvalid document!
Regarding EMS Operations and CIC Print Name, be sure you don't make any errors here. Both of these are the most important ones in the file.
Step 3: Make certain your details are right and press "Done" to progress further. After creating a7-day free trial account here, it will be possible to download new york state c4 forms or send it via email right off. The PDF form will also be accessible from your personal account page with all your edits. Here at FormsPal, we endeavor to ensure that your details are maintained private.